PCR TESTS NOT DESIGNED FOR DIAGNOSIS
In other words, I’m saying….
- The PCR test cannot be used alone to diagnose COVID-19
- A “case” is more than a positive PCR test
- COVID-19 in 2020-21 likely played the role previously played by severe influenza as a cause of excess mortality
- A positive PCR test alone should not be used to direct public health policy
Claim 1: “The PCR tests used to diagnose SARS-CoV-2 infections were never designed to do that, and the documentation inside each test says that; and the CDC has stopped using them because they can’t tell the difference between SARS-CoV-2 and influenza.”
NH Counterclaim: “PCR tests were absolutely designed to be used in this way and it’s how researchers have been using them for decades,” said Dr Campbell. “The patent document for PCR makes it clear that the inventors recognised the value of the technique in determining the presence of pathogens.”
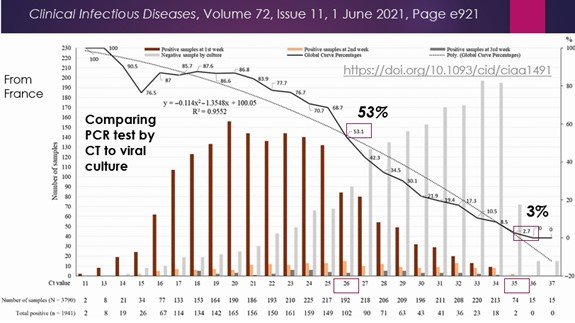
DrPC: PCR tests are designed to detect nucleic acid material, DNA or RNA (which is then reverse transcribed to DNA for the purpose of this test). What Kary Mullis had specifically warned is that the presence of nucleic acid material does NOT in and of itself determine the presence of disease, or even of infection. It is well known that the cycle threshold (CT), or measure of the number of amplifications of initial genetic material required to produce detectable immunofluorescence is critical to determining if viral material is even present. (R1) Studies have shown that even at a CT of 26, only 53% of the time can virus be successfully cultured. (R2) Even Dr Fauci, as Director of the USA’s National Institute of Allergy and Infectious Disease has noted that “[verbatim] any viral material detected at CT>35 is not going to be ‘replication competent,’ i.e. capable of causing infection or transmission.” (R3)
Since we know that the NZ Ministry of Health has determined that a CT of 40 or fewer is considered positive (R4), it can be expected that many “positive” tests will not contain viral material capable of causing either infection or transmission of disease. This leaves aside the issue, well known, that PCR tests can also measure “positive” for weeks after an individual has recovered from COVID-19. (R5)
An international consortium of 22 life scientists have published their investigation into the Corman-Drosten paper which is the basis for the world’s use of the RT-PCR test with respect to the SARS-CoV2 virus. (R6) The authors detected 10 molecular or methodological errors that were expected to increase the extent of false positive tests and raised questions about the validity of the test itself. They revealed undisclosed conflicts of interest by the authors as well as an otherwise unexplained short timescale (24hrs) between manuscript submission and acceptance at a time when only 6 COVID-19 deaths worldwide had been confirmed. This suggests that something equivalent to “insider trading” in the scientific world has likely occurred.
NH: “The first page of the insert that comes with every PCR test says it is “intended for the qualitative detection of nucleic acid from the SARS-CoV-2.”
DrPC: Indeed, it is intended to detect presence or absence of nucleic acid components, purported to be from a virus named SARS-CoV-2. However that does not mean it is capable of reliably diagnosing a clinical condition or even infection. The insert states that “… clinical correlation with patient history and other diagnostic information is necessary to determine patient infection status. Positive results do not rule out bacterial infection or co-infection with other viruses.”
NH: “One of the inventors, Kary Mullis, later went on to express a range of views contrary to mainstream science – including that HIV didn’t cause AIDS and the ozone hole didn’t exist.”
DrPC: Is this relevant or even true as stated or is this simply a deflection intended to impugn the inventor of the PCR test without the burden of having to address the points made? Does dissent from “mainstream science” mean it’s wrong? I believe that Professor Einstein might have disagreed.
NH: “As for the CDC, Dr Campbell says Dr Canaday’s claim isn’t true. Currently if a patient has symptoms but tests negative for COVID-19, a second test can be done to see if they’re caused by the flu. The CDC is now encouraging healthcare staff to use a test that can identify both to save time and resources.”
DrPC: As I mentioned, CDC has now accepted and has approved submissions from clinical laboratories to support the development of a “multiplex” RT-PCR test that would detect presence or absence of nucleic acid components of both the SARS-CoV-2 and influenza viruses. (R7)
NH: “It is not remotely accurate that the CDC test doesn’t differentiate between flu and SARS-CoV-2” Kelly Wroblewski, director of infectious disease programs at the Association of Public Health Laboratories, said in July. “It doesn’t detect influenza. It only detects SARS-CoV-2.”
DrPC: As noted above in the insert for the Quest qualitative diagnostic RT-PCR test used in NZ, there is a very clear statement that coinfection with other bacteria or viruses [such as influenza] may be present with a positive (or negative) test for SARS-CoV-2. A positive test for SARS-CoV2 at a cycle threshold of 40 may not contain sufficient viral load to cause disease, but coinfection with a significantly greater viral load of influenza virus may be the cause of the disease for which testing was obtained in the setting of a sick patient.
It is only by testing RT-PCR for the influenza virus, however, that one would know that. Indeed, the symptoms of COVID-19 show large overlap with the symptoms of influenza infection, and these, along with others, are often lumped together as “influenza-like illnesses” or ILI.
During the current pandemic, we have seen laboratory-tested cases of influenza plummet, by more than 99% (0.06% vs 13.7%) compared to a comparable period in prior years. (R8) And, as so often happens, if it’s been replaced by something else, you’re unlikely to find it, and if you don’t look for it, you’ll definitely not find it.
SUMMARY AND IMPLICATIONS
We hear so much about the increasing number of “cases” of COVID-19, especially now with the known contagiousness of the delta variant. But what is a “case”? As physicians and other health care practitioners who have actual experience treating patients know implicitly, a positive test is not a “case.” A “case” is an individual who is sick enough to come to the attention of the health care system.
For public health authorities and principals in government, calling something a “case,” while inaccurate, is much less cumbersome than “a-person-with-a-positive-test-who-may-have-no-symptoms-and-have-no-disease-or-ability-to-transmit-disease-or-may-have ability-to-transmit-disease-or-may-have-mild-symptoms-or-may-be-sick-enough-to-seek-medical-attention-or-may-be-hospitalised-or-sick-enough-to-be-in-intensive-care-or-may-require-a-mechanical-ventilator-or-may-be-at-risk-of-dying-from-COVID-19-or-may-have-died-of-COVID-19.” There is very limited data from the New Zealand Ministry of Health on the current mix of cases “types” or the presence of any co-existing disease during the current outbreak.
In this response, I have intentionally side-stepped the question of whether SARS-CoV2 exists as a virus capable of being isolated in its pure form, cultured in its pure form, and capable of supporting classical Koch’s postulates as a necessary definition of a pathogenic agent (i.e. a biologic entity that can reproducibly be proven to cause disease). This topic however is discussed in detail here. In the current context, however, a definitive answer to these questions is not necessary to discharge the validity of the PCR test in the way it is currently used.
Further commentary on COVID-19 and the PCR test by a NZ research physician can be accessed at: https://drsambailey.com/2021/08/07/what-is-covid19-and-where-is-the-pandemic/
References:
R1: Kary Mullis on PCR for HIV, 1993. https://youtu.be/_vVqlEKI95U
R2: Jafaar et al. on growth of SARS-CoV-2 at differing PCR cycle thresholds. https://doi.org/10.1093/cid/ciaa1491
R3: Dr Fauci on Cycle Threshold> 35. https://www.youtube.com/watch?v=A867t1JbIrs
R4: MOH statement on cycle threshold in NZ. https://d.docs.live.net/3f7813f2ac71c836/Documents/NZ%20COVID-%20Voices%20for%20Freedom/NewsHub%20response/MOH%20Letter_26_jan_2021_covid-19_cycle_threshold_value_for_pcr_testing_0.pdf
R5: Testing positive (PCR) after recovery from COVID-19. https://wi.mit.edu/news/new-research-reveals-why-some-patients-may-test-positive-covid-19-long-after-recovery
R6: Scientists review claims of PCR test for COVID-19 in Corman Drosten paper. https://cormandrostenreview.com/icsls/
R7: CDC guidance on multiplex PCR assays for SARS-CoV-2 and influenza. https://www.cdc.gov/coronavirus/2019-ncov/lab/multiplex.html
R8: Comparison of influenza positive testing in Southern Hemisphere countries in April-July 2020 to 2017-2019. https://www.cdc.gov/mmwr/volumes/69/wr/mm6937a6.htm?s_cid=mm6937a6_w
