NZDSOS Refutes Statements Made by Prof Graham Le Gros

NZDSOS Open Letter to Commissioners Refutes Statements Made by Prof Graham Le Gros
August 11, 2025
Dear Commissioners,
NZDSOS Concerns Regarding Statements Made by Prof Graham Le Gros
We watched and listened with interest to the testimony of Prof Graham Le Gros at the public hearings of the Royal Commission on 10 July 2025. It is not often that officials aligned with the government narrative are questioned about their understanding of aspects of the covid response, particularly in relation to the vaccinations administered to New Zealanders.
As per our email of concern to you on July 25, 2025 we disagree with a number of statements by Professor Graham Le Gros and are concerned that they could mislead the Commission. We suggest that all statements to the Commission are thoroughly investigated for validity.
Attached/below is our commentary under 13 headings regarding statements which we assess as misleading or incomplete.
We have not provided a list of references for this document as the other work provided to the Commission is heavily referenced. However, we are very happy and willing to provide additional references as needed to back up any of our comments.
1) High lethality, young doctors
Prof Le Gros stated that we knew c-19 had a high lethality and that it wasn’t just killing old, sick, immune suppressed people, but also killing young doctors, and that we needed a vaccine as quick as possible.
We disagree and note that very early in 2020 it was known/determined that the infection fatality rate was similar to an influenza-like illness and that it was the frail, elderly and co-morbid who were at most risk. The average age of death was 82 years which is older than average life expectancy.
In the UK, covid was downgraded from a High Consequence Infectious Disease (HCID) on 19 March 2020.
In NZ a Memorandum of Understanding between the Ministry of Health and Office of the Chief Coroner dated 18 Mar 2020 noted “According to the Director of Public Health, COVID-19 does not have a particularly high mortality rate and it is not particularly transmissible.”
John Ioannidis, a world leading epidemiologist, wrote a paper in May 2020 (published Oct 2020) setting out the infection fatality rate (IFR) from c-19 during the period before vaccines with the allegedly more serious variants. His calculation was that c-19 had an IFR less than 0.2% in most locations. In a later paper, he estimated the IFR for those aged 0 to 69 in high income countries to be to be 0.098% That is 99.9% of those under 70 years of age would survive a c-19 infection. These death rates would have been further reduced by improvements in treatment.
Yes, we agree that there were reports of younger doctors dying with/from c-19 early on. However without knowing more clinical details such as background health status, symptoms, how diagnosis was made (eg number of cycles used with PCR), what treatments were used, incentives for classifying death as due to c-19, it is hard to know what to make of these reports.
In the UK, further investigation suggested many of the deaths of healthcare workers were in darker skinned individuals and likely related to low vitamin D status and other co-morbid conditions, not merely age. Overall, young doctors with optimal vitamin D status and without co-morbidities were not at significant risk from c-19 infection. Meanwhile, since the mRNA rollout, many doctors have suffered from vaccine injury including unusual and aggressive cancers and sudden death.
We do not agree that a vaccine was needed as soon as possible. There were many things an individual could do to lower their risk of a poor outcome if/when they caught c-19. For the majority of otherwise healthy people, c-19 infection needed a few days of rest and supportive care including use of vitamin C, vitamin D, zinc and other nutrients associated with optimal immune function.
If more was needed, there were effective treatments being used overseas that could have been used equally well here if not taken out of the hands of doctors and other health practitioners e.g. Artemesia, hydroxychloroquine, ivermectin.
2) Vaccine development and clinical trial
Prof Le Gros suggested that vaccine development wasn’t sped up and that there were well done clinical trials that showed how that vaccine worked, what it delivered, and how safe it was.
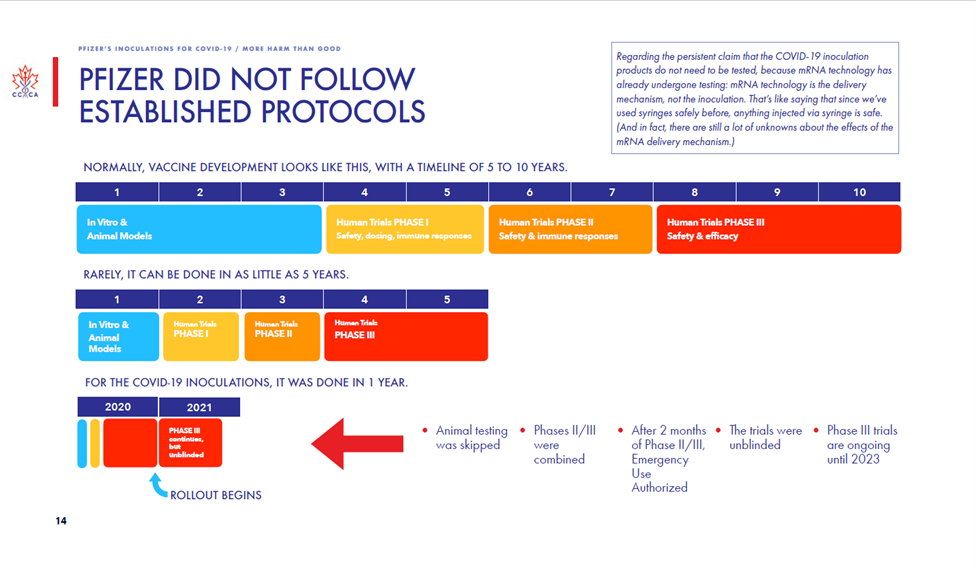
We disagree and note that the vaccine development timeline was significantly compressed. There is no substitute for time when observing efficacy and adverse effects. Having only two months of trial safety data and the outcomes of only 170 participants (out of approx. 44,000) before provisional approval is woefully inadequate for a medication that is to be used on the whole healthy global population.
The Canadian Covid Care Alliance has produced a useful slide and video addressing the shortening of the vaccine development process.
Prof Le Gros said: ‘Then it’s tested in cells, tested in mice, … to test whether it does integrate with DNA.’ We understand animal testing was minimal and the Medsafe datasheet specifically says Carcinogenicity and Genotoxicity were not studied. We would be interested to see the studies Prof Le Gros is referring to regarding DNA integration. We are aware of an in vitro (cell culture) study which did show integration of vaccine RNA into liver cells within 6 hours.
More recently scientists and researchers have found evidence that mRNA injections can induce widespread, long-lasting gene expression chaos with disruption to thousands of genes including those involved with mitochondrial (energy production) function, protein folding and quality control, DNA repair and genomic stability, immune system regulation and tumour suppression pathways.
With regard to vaccine safety and efficacy prior to approval, in its Clinical Evaluation document from January 2021, Medsafe was aware the efficacy was < 1%.
“Benefit
The randomised Phase 2/3 Study C4591001 shows that for participants without evidence of SARS-CoV-2 infection before and during vaccination regimen, from 7 days after the second dose, there were the following cases of symptomatic laboratory-confirmed COVID-19 of any severity:
- 8 (out of 18,198; 0.04%) in the BNT162b2 group and
- 162 (out of 18,325; 0.9%) in the placebo group.”
Medsafe was also aware that severe adverse effects occurred in 1.2% of vaccine recipients (compared with half that – 0.6% – in the placebo group). This is a completely unacceptable level of severe adverse effects to expect from a product to be administered to all healthy people.
“Severe AEs were reported in 1.2% of the vaccine group compared to 0.6% of the (saline) placebo group.”
In addition Medsafe noted a list of uncertainties, including the particularly relevant lack of evidence for prevention of transmission which was the basis of later mandates.
Uncertainties
Medsafe noted the Pfizer clinical trial was not designed or sufficiently powered to address all of the following uncertainties.
- It is not clear that the method of administration of the Comirnaty vaccine, as described in the datasheet’s ‘Special precautions for disposal and other handling’ section, is similar to the method of administration in the pivotal study.
- The duration of vaccine protection has not been established beyond two months.
- At this stage, there is limited evidence of protection against severe disease.
- There is no long-term safety follow-up information.
- Vaccine prevention of asymptomatic infection and disease transmission has not been established.
At this stage there is no information regarding vaccine effectiveness regarding:
- new variant virus lineages that may become important epidemiologically (including the possibility of change because of vaccine-selection pressures)
- immunocompromised people, and for pregnant women
- Pacific and Asian populations
- subjects with evidence of prior COVID-19 infection at baseline.
These features meant that following the initial risk-benefit analysis Medsafe was unable to approve it.
When asked under OIA (H2025061396) for the updated risk-benefit analysis which should have been done as new information came to light, Medsafe implied that no further risk-benefit analyses were undertaken.
“In Jul 2024 you provided a response to an OIA request regarding risk-benefit analysis for Pfizer covid vaccination prior to provisional approval. H2024045271 Please can you provide all the updated risk-benefit analyses that Medsafe has conducted as new safety and efficacy data has been published since the original provisional consent was granted.”
Medsafe conducts full risk benefit analyses when new safety data indicates it is significant enough to warrant it. For example, the new side effect of myocarditis associated with Comirnaty, the COVID-19 Vaccine Independent Safety Monitoring Board (ISMB) confirmed that this new side effect did not affect the risk-benefit profile, therefore an updated analysis was not necessary.
Your request is therefore refused under section 18(e) of the Act. Please see further information on the ISMB and its functions on the Health New Zealand – Te Whatu Ora website here:
https://www.tewhatuora.govt.nz/search?keywords=ismb.%E2%80%9D
In addition to the extremely limited data showing poor efficacy, high levels of severe adverse effects and many uncertainties, there were significant concerns about the integrity of the Pfizer trial raised by one of the site managers – Brook Jackson working for Ventavia.
We disagree with Prof Le Gros’ understanding of the vaccine clinical trial process and outcome and encourage the Commissioners to review the data Medsafe had access to prior to vaccine approval in Feb 2021.
He did note that in real-time New Zealanders were a part of that whole vaccine development process (i.e. the experiment). We do agree with this – that an experimental product was being administered (often with coercion and woefully inadequate information) to New Zealand citizens. As medical doctors we find this abhorrent.
3) Nature of the Vaccine: New technology – mRNA and lipids
Prof Le Gros has a very different interpretation/understanding of the nature of the Pfizer vaccine than we do. Our position is that mRNA technology has been studied in laboratory settings for several decades mostly in an attempt to treat genetic diseases or cancer but that no useful or approved products have ever been brought to market prior to the covid injections because of difficulties with the technology. If Prof Le Gros is able to provide data on any mRNA therapeutic which has seen wide-spread clinical use, we would be very interested to hear about it.
In the Risk Factors section of their Registration Statement with the US Securities and Exchange Commission dated 9 Sept 2019, BioNTech note the following:
“No mRNA immunotherapy has been approved, and none may ever be approved. mRNA drug development has substantial clinical development and regulatory risks due to the novel and unprecedented nature of this new category of therapeutics.” p 22
“As a potential new category of therapeutics, to our knowledge, no mRNA immunotherapies have been approved to date by the FDA, EMA or other regulatory agency.” p 22
“To date, there has never been a Phase 3 trial for an mRNA-based product or a commercialized mRNA-based product.” p 22
“Currently, mRNA is considered a gene therapy product by the FDA. Unlike certain gene therapies that irreversibly alter cell DNA and may cause certain side effects, mRNA-based medicines are designed not to irreversibly change cell DNA.” p 23
mRNA
The Pfizer vaccines are introducing synthetic modified genetic material (along with contamination with residual DNA) into the human body and causing human cells to produce foreign proteins.
Native human mRNA is fragile and quickly degraded as Prof Le Gros stated but the mRNA in the Pfizer product is not natural and has several modifications.
Pfizer Vaccine mRNA:
- Contains a genetic sequence from human alpha globulin so it can evade the immune defences and get into cells
- Uses methyl-pseudouridine to replace uridine which increases its stability and hence its persistence in the body, meaning spike protein will be produced for longer
- Has a Poly(A) tail (large numbers of adenine nucleotides at the end of the mRNA) to increase the amount of spike protein produced
- Is guanine-rich (has an increased proportion of guanine nucleotides) which makes it more stable
- Is contained within highly inflammatory lipid nanoparticles which are designed to disperse widely throughout the body
- Creates a protein that has two proline substitutions which change its conformation improving its stability
These modifications mean that the vaccine-induced spike protein is not the same (in amount, location, structure, duration of production or persistence) as the naturally occurring spike protein from infection.
He suggested that the mRNA product is very pure and makes only the required protein and nothing else. We do not agree with this statement. Medsafe’s original provisional consent had condition 5 noting the presence of ‘truncated and modified mRNA species present in the finished product’. Medsafe expected Pfizer to provide more information about the potential of these sequences of mRNA to produce other peptides or proteins that might be similar to human proteins and cause molecular mimicry and autoimmune conditions. It has not been possible to find out the outcome of condition 5.
In addition it has been discovered that the product is heavily contaminated with residual DNA from the Process 2 manufacturing. Dr Kevin McKernan has presented extensively on this topic.
Lipids
Prof Le Gros stated that the lipid used was ‘also an old technology’ and ‘just a normal lipid’ and implied it would just join the building blocks of the body like butter or mutton fat.
In contrast, the Medsafe Non-Clinical Evaluation document refers to two novel lipids – ALC-0135 and ALC-0159. It notes that two conventional lipids are also present in the vaccine.
“The active vaccine ingredient is encapsulated in a lipid layer composed of four lipids, two novel lipids (ALC-0315, ALC-0159) and two conventional ones, (DSPC, and cholesterol).” P 10/59
The safety datasheets for these novel lipids state they are for research purposes only and not for use in animals or humans.
ALC-0159
Echelon Biosciences Ltd (23 July 2021)
For research use only. Not intended for diagnostic or therapeutic use.
This product is manufactured and shipped only in small quantities, intended for research and development in a laboratory…
Cayman Chemical (18 Sept 2023)
THIS PRODUCT IS FOR RESEARCH ONLY – NOT FOR HUMAN OR VETERINARY DIAGNOSTIC OR THERAPEUTIC USE.
ALC-0315
Cayman Chemical (12 Aug 2024)
THIS PRODUCT IS FOR RESEARCH ONLY – NOT FOR HUMAN OR VETERINARY DIAGNOSTIC OR THERAPEUTIC USE.
Med Chem Express
Caution: Product has not been fully validated for medical applications. For research use only.
Gene therapy
It is our contention that the mRNA vaccines should have been considered gene therapies and should have been assessed under the Hazardous Substances and New Organisms Act.
The Medsafe datasheet for the adenoviral DNA Astra Zeneca vaccine noted that it was considered a GMO in some jurisdictions but through semantics avoided being considered one in NZ.
“This product contains genetically modified organisms (GMOs) under GMO regulations in other jurisdictions. Please note that under the Hazardous Substances and New Organisms (HSNO) Act 1996, this product is not considered to be an organism, and is therefore is [sic] not considered a GMO in New Zealand.”
Presumably a similar loophole allowed the Pfizer vaccine to escape scrutiny by HSNO Act.
4) Biodistribution
There seemed to be some confusion about the biodistribution studies with Prof Le Gros suggesting that studies using a tracer to understand the distribution of the LNPs had been misinterpreted. Our understanding is that biodistribution studies were done using LNPs and a tracer (either radiolabelled or luciferase expressing) rather than the spike-encoding mRNA. The purpose of these studies was to determine where the LNPs would take the mRNA. The study only lasted 48 hours and at that time tracer had not reached a peak at several sites. However, it did demonstrate the widespread distribution of the LNPs (with the assumption that the mRNA would go where the LNPs go).
5) Mechanism of action
Prof Le Gros noted that cells displaying spike protein on their surface became targets of the immune system and were destroyed, but when asked if this was a problem, he did not answer directly. Instead he deflected to suggest that only specialised immune cells (dendritic cells) take up the vaccine, produce spike protein and get delivered to the local lymph node where an immune response is generated.
Our understanding is that, following intramuscular injection, the lipid nanoparticles deliver the vaccine via the blood stream widely throughout the body. The cells of any or many organs then take up the mRNA and start producing spike protein. When they do so they are targeted for destruction by the immune system, and this means a wide variety of symptoms can manifest depending on which tissue or organ is affected.
The cells lining blood vessels (endothelial cells) in particular take up the vaccine making them targets of immune attack which can lead to clotting within, weakening of the wall of, or rupture of the blood vessel. Symptoms will depend on which blood vessels are affected – stroke, pulmonary embolus, ruptured aorta, heart attack. Pathology work done by Dr Arne Burkhardt demonstrates this occurring, especially when staining for spike protein is used.
In addition to blood vessel cells expressing spike protein, other tissue cells such as heart muscle cells, brain cells, connective tissue cells, can also take up mRNA and produce and express spike protein. They are then potentially targets of the immune system.
Prof Le Gros stated that the mRNA is very quickly degraded within minutes to an hour and noted that the (spike) protein lasts a lot longer. He did not provide evidence for the former statement nor any information about how long the protein would last. We point out that studies have shown the persistence of vaccine mRNA for several weeks in various tissues (much longer than minutes to an hour) and a recent study has shown persistence of spike protein in some people out to 700 days post last vaccination which is when the research ended.
We agree that native mRNA is transient and does not last long, however vaccine mRNA is synthetic with modifications to ensure persistence.
Prof Le Gros also mentioned several times that the purpose of vaccination was for the body to make neutralising antibodies against the spike protein which would protect against the virus. This is correct in theory, but we note in the real world that the presence of vaccine-induced antibodies against spike protein has not conferred immunity or protected against c-19 infection.
6) Measles Vaccine
When asked if he had any comments about the idea that the Pfizer c-19 vaccine was not a vaccine but an injection of genetic material, Prof Le Gros suggested that measles vaccine was similar and contained RNA and the ability to transcribe things. He said it was mischievous to state that the c-19 vaccine was an injection of genetic material.
We stand by our statements that the Pfizer vaccine is an injection of synthetic genetic material and is very different from any previous vaccine administered to healthy people. We think likening the measles vaccine to the Pfizer mRNA covid injections is not just mischievous, but incorrect and highly misleading.
Measles is caused by a single stranded RNA virus (Morbillivirus hominis). The two brands of vaccine in NZ use weakened strains of various measles, mumps and rubella viruses grown in chick embryos or human derived cell cultures. The whole weakened virus contains native/natural viral RNA which has not been synthetically modified to include an alternative nucleotide, or other alterations made that make it persist or increase foreign protein production. The measles vaccines enable the measles virus to reproduce in human cells but not manufacture an isolated synthetic foreign protein.
In addition the measles vaccine does not use lipid nanoparticles to aid widespread distribution.
Other vaccines such as Engerix-B against Hepatitis B and Gardasil against Human Papilloma Virus use genetic modification (relevant proteins or virus-like particles are made in yeast – Saccharomyces cerevisiae – cells) in their creation, but the injections themselves do not contain synthetic genetic material designed to make human cells produce a foreign protein.
7) Manufacturing of vaccine
Prof Le Gros appears to have confidence in the manufacturing process and monitoring of production. We do not share his confidence. He believes the Pfizer vaccine has undergone stringent, robust testing before being approved and ongoing stringent testing of batches as they are released.
We would point out that until Nov 2023 Pfizer’s Comirnaty only had provisional consent in NZ which has NO REQUIREMENT for safety, efficacy or quality reports. According to the Gazette notice, there were 58 conditions most of which were the requirement for Pfizer to provide additional data. The outcomes of these conditions have been deemed ‘commercially sensitive’ and not shared with the public.
The RMP noted much missing information, the Medsafe datasheet also pointed to the lack of data in certain areas e.g. no testing for genotoxicity or carcinogenicity was conducted. No independent testing of the product was done in NZ despite the population being assured that this would be done.
He acknowledges that plasmid DNA is present during production but assumed it has been purified away. This is not the case in any of the vials examined independently which have been shown to be grossly contaminated with DNA. According to Dr Kevin McKernan who the Commissioners have heard from, the enzymes which are specific for DNA do break up the DNA but have not removed it and have made it more dangerous by chopping it into a large number of smaller pieces which all have the potential to integrate.
Prof Le Gros was dismissive about the harm caused by SV40 contamination in the polio vaccine of the 1960s. It is our understanding that this historic contamination has been associated with certain cancers (primary brain cancers, primary bone cancers, malignant mesothelioma, and non-Hodgkin’s lymphoma) in recipients many years down the track.
SV40 is used in the laboratory to induce tumours in experimental animals.
It is our assessment that with Comirnaty, rather than our regulatory authorities tending to put more and more controls in place, they have basically given this highly risky product a free pass with minimal scrutiny and have not acted to recall it when significant alarm signals have been raised.
Regarding evaluation of the manufacturing sites, we would be interested to know how they were assessed for adherence to GMP (Good Manufacturing Practice). Prof Le Gros believes ‘the drug companies that were being commissioned to make the vaccine were being rigorously tested and evaluated’. We note that the original Comirnaty product used in NZ lists one manufacturer on the Gazette notice.
Manufacturer: Pfizer Manufacturing Belgium NV, Puurs, Belgium
But by Oct 2023 when the Gazette notice lists six different versions of Comirnaty, the number of manufacturing sites had increased significantly.
Manufacturers: Novartis Pharma Stein AG, Stein, Switzerland
Pfizer Manufacturing Belgium NV, Puurs-Sint-Amands, Belgium
Sanofi-Aventis Deutschland GmbH, Frankfurt am Main, Germany
Baxter Oncology GmbH, Halle-Kunsebeck Westfalen, Germany
Patheon Italia S.p.A, Milan, Italy
Polymun Scientific Immunobiologische Forschung GmbH, Klosterneuburg, Austria
Siegfried Hameln GmbH, Hameln, Germany
Delpharm Saint Remy, Saint Remy Sur Avre, France
Catalent Anagni SRL, Anagni, Italy
BioNTech Manufacturing Marburg GmbH, Marburg, Germany
Mibe GmbH Arzneimittel, Brehna, Germany
Allergopharma GmbH & Co. KG, Reinbek, Germany
Where is the Medsafe assessment of all these manufacturing sites?
8) Process 1 and Process 2
Prof Le Gros seemed unsure about the two different processes used in manufacturing the vaccine: Process 1 using PCR technology to make smaller batches of the substance used in the clinical trials and Process 2 using DNA and bacterial plasmids to manufacture at scale the product that was injected into New Zealanders.
It is our position that when such a significant change in manufacturing process occurs, it requires a separate clinical trial. It is unscientific and unethical to assume products made by quite different processes are the same or similar.
9) Adverse events/pharmacovigilance
Prof Le Gros is a scientist not a medical doctor and so is somewhat removed from patients and their clinical histories. Pharmacovigilance and safety monitoring is not his area of expertise and, perhaps rightly, he was reluctant to get into the details of vaccine safety and adverse reactions, even though vaccine safety was the topic of that day’s hearings.
As doctors, vaccine harm (lack of safety) was, and is, the main focus of our concern.
He was aware viral infections can have quite tragic sequelae 10 years later but did not apply that same logic to novel medical products. There are multiple examples of early enthusiasm for medicines followed by demonstration of significant harm later on.
His expressed understanding of the risks of infection versus injection are the opposite of ours. ‘I fear the long term effects of COVID, far more than the long term effects of the vaccine.’
He stated the vaccine stimulates an immune response in the arm, and draining lymph node, and that’s as far as it goes. In contrast, he stated the c-19 infection gets inside a person and affects all the cells lining the blood vessels, of the kidneys, of the heart, of the brain.
We say it is the other way round! The infection is limited to the mucosal surfaces of upper airways for the vast majority of people and immune defence prevents further incursion, whereas the vaccine is distributed far and wide throughout the body of everyone injected thanks to the LNPs.
The presence of virus in wastewater samples was used as evidence that the virus goes everywhere in the body. We don’t know the details of how wastewater testing is done but do know that PCR tests with ramped up cycles will find almost anything, so the significance of this is not clear without more information. We would also say that the human body has many ways of excreting unwanted substances and just because something is being excreted does not mean it has caused disease.
Our view is the vaccine has caused widespread damage to many individuals because the mRNA has been taken up by a variety of tissues and is producing large amounts of spike protein and in some, that spike protein production may be ongoing. The immune system is overwhelmed responding to this and we have seen raised and disproportionate levels of IgG4 and very high spike antibody levels in some people several years following most recent injection.
The issue of DNA contamination is also likely contributing to the widespread harm we are witnessing, particularly with the increase in rare and aggressive, rapidly progressive cancer diagnoses.
We do not disagree that some individuals have been severely affected by covid infection but would consider these to be in the minority and most will have significant co-morbidities and/or be very elderly.
He stated that ‘the virus really does cause cardiac inflammation’ but was reluctant to concede that the vaccine could cause myocarditis. He wanted to wait for more evidence. ‘Time will tell and information will come in the future to see whether there’s actually plausible or causal links. Let’s just wait.’
We say the alarm bells are ringing, numerous people have already been significantly adversely affected by myocarditis secondary to the vaccine and a number of otherwise healthy people have died. The published NZ Myocarditis Study demonstrates this. As clinicians, it is our position that we should not ‘just wait’, there is more than enough evidence of harm already to stop further injections.
We have asked for evidence of myocarditis secondary to covid infection in NZ under OIA and were advised by Health NZ no cases could be found. We appreciate that this does not mean there are no cases due to the way data is collected, but evidence of cases of myocarditis due to covid infection needs to be provided and reviewed.
Prof Le Gros was somewhat dismissive of other adverse reactions suggesting they may just be a bruise or a red spot or feeling dizzy for a week. Those symptoms could indicate serious conditions and without thorough causality assessment, it is not possible to know whether they are minor or serious.
He appeared to have confidence in New Zealand’s pharmacovigilance systems which we believe is unwarranted. This is one of our major concerns as we do not believe that pharmacovigilance is robust or thorough. Many adverse events following vaccination are not being reported to CARM and those that are, are not being assessed for causality.
Many people are being advised by their treating doctors they have ‘anxiety’ when they likely have significant diagnoses. When they ask whether the vaccine could have caused their condition, they are told “Oh no, it won’t be the vaccine”.
A case in point is the young man Jason Cluley who presented immediately before us at the public hearing. He had suffered cardiac symptoms then a cardiac arrest within a few months of his second vaccine. He now has an implanted defibrillator which has had to shock him out of a life-threatening arrhythmia 3 times in the past year.
When he asked his doctors, they told him it was nothing to do with the vaccine and it was due to covid or some other virus. However, he didn’t have covid until 2023. If no-one has considered this related to the vaccine, it is likely a CARM report has not been done. How many other New Zealanders have similar stories and are not counted in any official numbers?
It should be pointed out that Medsafe’s last published safety report in Nov 2022 had 3688 serious events recorded as well as 184 deaths. There are likely to have been many more in the ensuing two and a half years.
It is disingenuous and wrong to suggest that the Pfizer mRNA vaccine is the ‘safest vaccine we’ve ever made’ and that its ‘safety profile compared to any other vaccine is amazing’. The adverse event and death reports in NZ and internationally are off the charts.
10) Censorship/debate
Prof Le Gros was asked whether he thought discussion and debate were shut down during the c-19 response. He did not directly answer this but when further questioned about whether it would be appropriate to shut down debate temporarily for the Greater Good, he replied yes, if the government was dealing with the right evidence.
We consider this a very dangerous position to take. The right evidence for what? Science progresses by discussion and debate and this should be encouraged not censored. Censorship of discussion creates an impression that the censoring side cannot defend or explain its position, so it is silencing ideas that it can’t respond to. It does not engender trust or confidence.
11) Anaphylaxis
It is good Prof Le Gros accepts long term illness following vaccination. This has been called Post Acute Vaccine Syndrome and is extensively documented, as the RCI has heard and must accept. Anaphylaxis IS documented in Medsafe’s Safety Reports, on the VAERS website, and in many other countries’ pharmacovigilance recording, as well as Pfizer’s own post marketing documents.
As an immunologist he should know that anaphylaxis is NOT mediated by IgA, but by IgE, an antibody class found in the blood, ready for immediate immune attack against antigens. IgA antibodies are found on membrane surfaces like the airway and the gut. It is these antibodies that are relevant to immunity against pathogens like SARS-CoV-2, rather than blood borne antibodies which the vaccines are supposed to stimulate.
12) Sources of information, medical literature
Prof Le Gros was asked whether he had come across papers that ostensibly raise concerns with the safety of the vaccine, and how he would make sure that he found and saw that information.
His response suggested he thought that those who had a different view or were concerned about vaccine safety were using sources of information that were not in the accepted or normal mainstream published literature.
As he correctly pointed out, there are hundreds of thousands, if not millions, of articles published about the covid response including regarding effects of vaccination and it is not possible for one person or one organisation to be across all of them.
We would like to reiterate that in our work, and in particular our letters to officials, we are in the main referencing peer-reviewed published medical and scientific literature, official government documents and OIA responses. Sometimes we refer to pre-prints or substack articles, almost always containing relevant references. Most of the latter are written by reputable scientists or journalists.
Prof Le Gros’ comment that those who don’t get published should ‘go back and argue their case’ does not address the bias of medical journal publishing. This is a whole huge topic in itself. Suffice it to say that scientific and medical journals have become mouthpieces for industry (including the pharmaceutical industry) which has significant control over what does and does not get published, including the escalation in article retractions since the pandemic. This has been commented on by several prominent medical journal editors such as Dr Marcia Angell former Editor in Chief of NEJM, Richard Horton former Editor in Chief of the Lancet and Dr Richard Smith and Fiona Godlee both former BMJ editors.
13) Conflicts of Interest
Prof Le Gros volunteered information regarding potential conflicts of interest and stated he was retired and not employed by anyone and had volunteer role(s).
He did note that one of the benefits of forming the Vaccine Alliance was ‘creating a pipeline of opportunity’ (presumably to make money).
Others have written comprehensively about what may be perceived as conflicts of interest. Professor Le Gros’ career history was outlined by Dr Ursula Edgington in an article written after his testimony to the RCI. He has connections to the US National Institutes of Health, World Health Organization and large European pharmaceutical companies. He is also listed as Director of four pharmaceutical companies including one linked to China, and he has benefited from large amounts of public money via the Malaghan Institute.
Thank you for reading our letter and for your attention to the points we have raised. The Commission is in a unique position to assess the accuracy of all statements presented during the inquiry critically. We trust that our commentary will be considered carefully as part of this important process, and we are happy to provide further supporting evidence if required.
Sincerely,

Drs Matt Shelton, Alison Goodwin and Cindy de Villiers
For and on behalf of NZDSOS Members
Watch: NZDSOS Video Response to the Royal Commission’s Witness Prof Graham Le Gros