Efeso Collins Coroner’s Report Under Scrutiny

The coroner has released her ruling on the death of Efeso Collins who died age 49 in February 2024 after competing in a Water Run event in Auckland.
“He died of natural causes, being cardiac disease arising from complications of diabetes, obesity and hypertension.”
We wrote to Coroner Anderson asking her to consider the role of covid vaccination in her deliberations. As an MP, Mr Collins would have been fully vaccinated and the coroner’s report notes he had had three covid vaccinations with the most recent being 5 March 2022.
We have read Coroner Anderson’s findings including the six paragraphs devoted to discussing and dismissing our concerns. We do not feel the assessment has been sufficiently thorough for her to be able to rule out a causal or contributory role of covid vaccination and there remain unanswered questions.
We appreciate that this is not a straightforward case and there are comorbidities to consider which may in fact account in full for Mr Collins’ death. However, an assessment in previous ‘normal’ times would have been more thorough.
Briefly, the inadequacies are as follows. These issues are not limited to the assessment of Mr Collins’ death. We’ll consider each point in more detail.
- Limited PM examination with no histology
- No consideration that the vaccine may have accelerated coronary artery disease
- No consideration that there could have been clinical or subclinical myocarditis with residual scarring as a focus for an arrhythmia
- No specific comment re cause of aortic valve abnormalities or possible endocarditis
- No pharmacovigilance process
- No comment re lack of data regarding covid vaccination in Pacific peoples, or re limited data in people with underlying cardiovascular disease
Limited PM examination with no histology
“A post-mortem examination consisting of a CT scan, external examination and toxicology/biochemistry testing was performed by a forensic pathologist.”
There was limited post mortem assessment in this case with only CT imaging, external examination of the body and testing of body fluids. This means that individual organs were not examined either with the naked eye or under the microscope. It is not possible to make a definitive diagnosis without histology. It is not possible to rule out previous myocarditis by post mortem CT examination.
Microscopic examination of the:
- coronary arteries could have revealed whether there was an acute blood clot, chronic narrowing, inflammation, dissection (splitting)
- heart muscle could have demonstrated whether there was an area of muscle death due to compromised blood supply, or evidence of previous inflammation with residual scarring
- aortic valve could have determined why it was heavily calcified (hardened and rough)
Even if ‘coronary artery disease’ is the actual cause of death, it should be noted that covid mRNA vaccination can contribute to this via inflammation of the vascular endothelium (cells lining the inside of the blood vessels). Acute then chronic inflammation can lead to fibrosis (scarring) and calcification of tissues.
Accelerated Coronary Artery Disease and Enlarged Heart
“Heavy calcification was identified in Fa’anānā’s aortic valve in his heart and his coronary arteries (the blood vessels to the heart). There was also borderline enlargement of his heart, rib fractures consistent with resuscitation injuries, and calcification in a pattern suggestive of diabetes.”
The CT scan has identified heavy coronary artery and aortic valve calcification in addition to enlargement of the heart.
Without further assessment it is not possible to say what caused these abnormalities with any certainty. The coroner has assumed that they are due to underlying cardiac risk factors of diabetes, hypertension and obesity (despite noting that these were well managed by his GP). We say they could be due to post inflammatory effects of covid vaccination.
Enlargement of the heart could be due to obesity or hypertension or cardiomyopathy (disease of the heart muscle) but without examination of the heart, it is not possible to say.
New, accelerated and/or difficult-to-treat hypertension has been noted in people post covid vaccination. This is thought to be due to changes to the compliance/elasticity of the arteries that the heart has to pump blood through, and/or autonomic (nervous system) damage to the reflexes that regulate the circulation.
An assessment of increased cardiovascular risk from the mRNA jabs was published back in 2022. Its author, cardiologist Dr Aseem Malholtra is still working, like us, to get this information out to the vulnerable masses 4 years later. His testimony to US Congress of June 2026 is here.
The covid vaccine used synthetic genetic material, designed to persist and not degrade quickly, to cause body cells to produce the foreign spike protein. It is now known that this spike protein production does not cease in some people. It is possible some may still make spike protein for the rest of their lives but this is not being tested for.
Myocarditis – Clinical or Subclinical
There is no information about whether Mr Collins experienced any side effects following his covid vaccinations. It is possible he had no noticeable adverse effects but it is also possible that he did experience some of the side effects many people experienced. Previously healthy people experiencing palpitations, shortness of breath, chest pain, fatigue were advised they were suffering from ‘anxiety’ and most were dismissed without investigation if they sought medical advice. However, these are symptoms of myocarditis and should be fully assessed. Even in the absence of these symptoms post-vaccination it is possible to experience sub clinical-myocarditis i.e. damage to the heart without knowing it.
Various studies have shown widespread heart damage post mRNA vaccination e.g.
- Thai boys study (Mansanguan) – 3.5% myo/pericarditis in boys after 2nd dose of Pfizer (this is 35 000 cases per million!)
- Japanese MRI study (Nakahara) – every patient with a first or second Pfizer dose within 6 months showed silent heart damage
- PULS score (Gundry) – this cardiologist’s patients showed worsened markers of coronary artery inflammation after injection
- Swiss cardiac marker study (Buergin) – 2.7% myo/pericarditis after first Moderna mRNA booster but all vaccinated had a small rise in troponin, signalling heart muscle cell damage
- Czech military study (Dlouhy) – 49% of fit recipients after 2nd covid mRNA jab showed transient elevation in a blood marker of heart failure
The description of his death – completing a physical challenge with no signs of distress or pain and then appearing fine and well afterwards, followed by a sudden collapse with ventricular fibrillation (VF) observed on the Automated External Defibrillator (AED) – suggests a sudden arrhythmia. Coronary artery disease (especially if inflammatory and accelerated) and acute ischaemia absolutely could cause this, but so could scarring from previous myocarditis. Without histological examination of the heart and coronary arteries it is not possible to say if either or both of these features and/or something else entirely were present.
Endocarditis
It is well recognised and acknowledged that the Pfizer vaccine can cause pericarditis and myocarditis. It is less recognised that the third (inner) layer of the heart – the endocardium – may also be damaged just as the inner lining of blood vessels (endothelium) can be damaged by the vaccine.
It is noted that a sister had had heart surgery in her 30s but no detail was provided. Valvular disease e.g. post rheumatic fever, is one reason for heart surgery at a young age. It is possible he had long standing valve disease but there is no record that there was any such pre-mortem diagnosis.
Pharmacovigilance
We do not have any information about whether Mr Collins’ premature death was reported to CARM or not. It should have been (and should still be) reported. If pharmacovigilance was being done appropriately and thoroughly, every death and (serious) adverse event in a vaccinated New Zealander would be causally assessed, using recognised criteria, for its potential relationship to covid vaccination and categorised on a scale from certain to impossible.
If such data is not collated and analysed, we will have no idea of the true scale of vaccine injury. We will not know whether the vaccine can contribute to acceleration of cardiovascular disease, or a variety of other conditions, in the years following vaccination. A normal vaccine or drug trial takes years before the products are used in humans on a wide scale. It is 5 years now since New Zealanders were first exposed to the gene technology which had extremely limited clinical trial data (a few months) when it received provisional consent in NZ. Our position is that abundant data from around the world has proven how unsafe and defective the genetic injections are.
It is incorrect to think that just because it was nearly 2 years post Mr Collins’ last vaccine, that the vaccine had nothing to do with his death. The product was a genetic injection, not a normal vaccine, and there is no prior experience with such products outside of advanced cancer to have any idea what medium and long term outcomes there could be. Monitoring should continue for decades, especially when no genotoxicity or carcinogenicity studies were undertaken. To be as polite as possible, it is extremely premature to be suggesting that the vaccine could not be causing ill effects only presenting several years down the track.
Lack of basic data in Pacific Island people
The Pfizer covid vaccine was not tested in Pacific Island people with their particular genetic makeup so it should be even more important that post marketing data in this group be collected and analysed.
Cardiologist commentary
Cardiologist Dr Tony Scott was asked to comment on our concerns. Effectively he dismissed the potential role of covid vaccination by saying an event nearly two years post vaccination was “well outside the time-frame of post vaccination myocarditis or other cardiac effects”. He also suggested that Mr Collins “was also outside the age group affected in the very rare cases”.
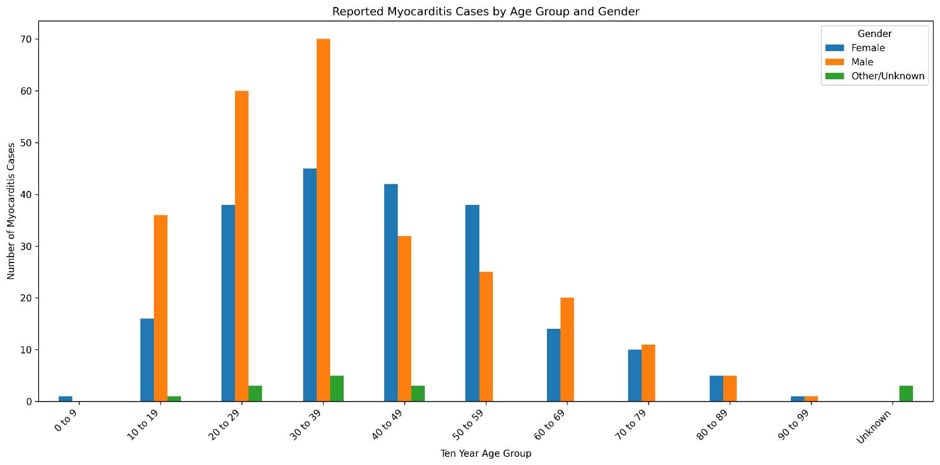
We disagree strongly with both these comments. As noted above, we are gaining some idea how long adverse events can occur post covid vaccination as the evidence is still being gathered. Although supposedly more common in younger people, myocarditis can affect people of all ages. An early CDC study showed markedly elevated rates in the 2 weeks after vaccination in all deciles up to the 50 to 60 year olds. Regarding the number of reports of myocarditis made to CARM, the highest number were in males age 30-39 with males age 40-49 having a substantial number of reports. [Note that this is not a rate adjusted for population size.] No-one is too old to get myocarditis.
Graph 1 Age and gender distribution of the NZ myocarditis cases reported to CARM by Nov 2022
There is no reference provided for the comment that “large registries do demonstrate a marked increase in out-of-hospital cardiac arrest burden tracking with Covid infection waves and healthcare system drain, rather than after vaccination rollouts”.
Conclusion
We get criticised for assuming every death in a vaccinated person should be put down as due to the vaccination. That is NOT what we have been stating at all. Rather we have been advocating for a thorough formal assessment of each death in a vaccinated person to determine whether the vaccine may have played a role especially when the death is sudden and very unusual.
We are disappointed with the low standards of investigation and lack of curiosity among our medical and legal colleagues. We continue to observe that anything to do with covid vaccination is swept under the carpet as rapidly and completely as possible.
A curious and thorough coroner would have asked about any post vaccine adverse effects, would have ensured reporting to CARM had occurred and expected a formal causality assessment to be completed by suitably qualified pharmacovigilance experts, and would have noted the limitations in her determination posed by lack of histological examination. Coroners must understand the chilling effect on pathologists that the Medical Council’s Guidance Statement had, being a thinly veiled threat against ethical doctors who disagreed that the injection could possibly be ‘a zero-risk medical product’, as defined by then MCNZ chairman Dr Curtis Walker.
The weight of medical evidence for suspecting vaccine causation in these type of deaths is strong, easily available and regularly presented by us to at least some coroners. They are lawyers who must understand the basic principles of liability, even if the fiduciary obligations to the deceased’s loved ones to explain the death fully have been pushed aside by covid era statute.
We provide a list of relevant references in our letter to Coroner van Son on the death of rugby star Connor Bachop here.