Documented Devastation: The Greatest Medical Crime in Human History

The Economics of Public Health
A basic tenet in public health is the association between economics and health. Wealthy populations tend to flourish and impoverished populations tend towards high rates of ill health and low life expectancy. A vicious cycle quickly establishes, with ill health causing loss of income and lost income leading to factors which exacerbate stress and disease.
Professor of Epidemiology at University College London, Michael Marmot is probably the leading researcher in this field of public health. As Chair of the World Health Organization (WHO) Commission on Social Determinants of Health, he co-authored Closing the Gap in a Generation, a report which explained the significance of social and economic policies on population health outcomes.
Until recently wealthy societies have been largely protected from the crushing intergenerational debt that health care expenses cause in poor nations. Political economist Dr Toby Rogers explains our modern day economic system as a business model of iatrogenic injury stripping wealth from the middle class. Similar evidence is presented by other economists such as Catherine Austin Fitts and Professor Richard Werner.
What the pharmaceutical-hospital industrial complex was smart to do, was to buy up everything and everybody … They bought up the mainstream media … all of them are taking huge amounts of money from the pharmaceutical industry. And they bought up the political system. So politicians wont ask questions. They bought up the regulators … They bought up continuing medical education so doctors are just trained by the pharmaceutical industry in the latest products they want to sell. They bought up universities, their curriculums for medical schools … They’ve bought up every step in the knowledge production process in science and medicine. ~ Dr Toby Rogers
Documented Devastation
In June 2026 the World Council for Health (WCH) published The Greatest Medical Catastrophe Nobody Wants to Name: What the Data Actually Shows About the Pfizer COVID Injections. Described as a “deep dive” presenting material which may be used in individual or class action legal steps, the article reviews five mortality analyses conducted by independent researchers, and a general overview of the harms caused by hospital protocols. This is our synopsis of the WCH article.
1. Diabolical Real World Data from World Health Organization
Perhaps the biggest bombshell of all is a paper by Okoro et al published in the International Journal of Risk & Safety in Medicine in April 2025. Using real world data from the WHO Covid-19 Dashboard, a clear and horrifying pattern of harm across geographical locations following the vaccine rollout emerges. Focused on covid deaths, this paper does not touch on the plethora of non-covid harms associated with these toxic products.
According to World Health Organization data, COVID-19 deaths increased with vaccination coverage by the following rates in each WHO region:
Africa: 43.3%
Eastern Mediterranean: 350.9%
South-East Asia: 403.7%
Europe: 496.5%
Americas: 705.9%
Western Pacific: 1,275.0%
New Zealand sits within the Western Pacific region.
Conclusion
“COVID-19 mortality increased in the vaccination era, especially in regions with higher vaccination coverage.“
These diabolical outcomes fly in the face of all claimed intent. The fact that such publications are obscured from public scrutiny through control of corporate media and medical literature whilst WHO continue to favour flawed research using mathematical models, is at the very least, sinister.
Okoro et al emphasise “the subjective nature and inherent biases in mathematical models” used deceitfully to claim illusory infection fatality rates and vaccine effectiveness. We have explained this deceit in a number of articles, for example here and here.
2. The Role of the Pandemic Response in Excess Mortality
WCH also reviewed the work of Professor Denis Rancourt et al, including their 2024 publication on excess all-cause mortality – see our review here; and their 2023 publication on vaccine associated mortality in the Southern Hemisphere – see our review here. Findings show 30.9 million excess deaths globally throughout 2020–2022 with three main causes: lockdown policies, medical protocols and “vaccine” rollouts. Over half of all excess mortality is attributed to vaccine-associated deaths.
The core finding in Rancourt et al’s research is that the pattern of excess mortality is incompatible with a spreading viral pathogen as the primary cause of death. New Zealand is one of nine Southern Hemisphere nations in which they find no detectable excess mortality until after the vaccine rollout, when deaths began to spike, especially in the 80+ year age group.
NZDSOS have written many letters to New Zealand authorities attempting to alert them to this atrocity. We are largely ignored or dismissed. The reasons for this are no doubt manifold and complicated, including disbelief that covert violence would be perpetrated on innocent people by “The Guards Who Love Us“. Catherine Austin Fitts shares these wise words in relation to this phenomenon.
3. Pfizer Claims Dismantled and the Untimely Death of a Whistleblower
Christine Cotton was a French biostatistician and clinical trials expert with a 25 year career working in the pharmaceutical industry. In a July 2023 conversation with documentary filmmaker James Patrick, she described violations of good clinical practices in the Pfizer covid vaccine trial.
In December 2024 Dr Cotton published a detailed 400+ page report exposing multiple issues including concealed data, incomplete results, methodological fraud, document falsification and more. Announcing the publication on social media, she referred to the covid vaccine as “the biggest scandal in the history of the pharmaceutical industry: lies, mass manipulation, refusal to acknowledge the victims…“
The World Council for Health analysis of Dr Cotton’s work outlines five main findings:
- The “measurement trick” of claimed efficacy.
- No proven efficacy against severe disease.
- No proven efficacy against death.
- Bait-and-switch between Process 1 in the trial and Process 2 in the mass-administered product, meaning zero data was available for the product administered in the global vaccine rollouts.
- Dr Cotton did not have access to Pfizer’s data showing underreported mortality in the vaccinated trial participants.
In January 2025 Dr Cotton filed a complaint against health authorities based on her findings. It was dismissed without investigation. In November 2025 she reported becoming unwell immediately after filing the complaint, and experiencing a range of worsening symptoms for which no diagnosis had been made, leading to a cascade of events including the loss of her dream home. She took her own life in June 2026, leaving a forensic trail of catastrophic population health harms in her wake.
4. Pfizer Data Exposed By Research Teams
Representing Public Health and Medical Professionals for Transparency, lawyers connected to the Informed Consent Action Network filed a request in the District Court of Fort Worth Texas, for the US Food and Drug Administration (FDA) to produce all of the documents submitted by Pfizer used by the FDA to license their COVID-19 vaccine. In January 2022 the District Court judge ordered the release of all documents in lots of 55,000 pages per month.
In response to such a large volume of technical documents, Dr Naomi Wolf made a public call for appropriately qualified volunteers to collaborate on data analysis via her media outlet, The Daily Clout. Over 3000 scientists, clinicians, data analysts, forensic investigators and other experts volunteered, forming six teams to investigate the data and produce independently peer reviewed reports named The Pfizer and Moderna Documents.
Over 100 reports reveal horrific outcomes known during the clinical trials for these products. The teams continue now as the Pandemic Investigation Project who have exposed that a higher rate of deaths was seen in the vaccine arm of the Pfizer trial, with delayed reporting used to obscure the data.
5. Multiple Concerns on Forensic Analysis
The final paper reviewed by WCH is Forensic Analysis of the 38 Subject Deaths in the 6-Month Interim Report of the Pfizer/BioNTech BNT162b2 mRNA Vaccine Clinical Trial, published in October 2023. A total of 38 deaths amongst 44,060 trial participants is only 17% of the expected number of deaths based on US age adjusted mortality. This may be explained by the fact that 4.2% of the randomised participants were “discontinued”, a number of whom appear to have died whilst many were completely lost to follow up.
Of the 38 documented deaths, 21 were vaccinated and 17 were unvaccinated, contradicting the “life saving” quality of the product. Fifteen of the deaths were either found dead, or died suddenly, twelve of whom were vaccinated against three in the placebo arm, also contradicting claims of lives saved.
WCH report the following key findings in this analysis, concluding that evidence suggests the trial was not properly conducted and that the product causes harm.
- No significant difference between the vaccinated and placebo arms in the trial during the placebo-controlled period.
- A 370% increase in cardiovascular deaths in the vaccinated arm compared with the placebo arm, which Pfizer did not disclose to the regulators.
- After the product was authorised, participants were unblinded and the placebo arm were offered the vaccine. Deaths in the unvaccinated arm slowed and plateaued, whilst the death rate amongst the vaccinated continued at the same rate.
- Systematic inconsistencies between the subject data listed in Pfizer’s 6-Month Interim Report and in publications based on this data, relating to death and adverse events. Regulatory agency and medical literature reviewers appear not to have detected these inconsistencies.
6. The Killing Fields of Hospital Protocols
The hospitals became death traps. Not because the virus was unstoppable, but because the standard of care was lethal.
Mechanical Ventilation
In April 2020 New York City based intensive care physician Dr Cameron Kyle-Sidell described the harms being caused by mechanical ventilation protocols. Ventilation was promoted by the World Health Organization who supported a ramp-up of mechanical ventilator production. It became quickly apparent that this was yet another public-private partnership focused on profits over evidence based health care.
Denial of Early Treatment
Until 2020 there was nothing controversial about offering early treatment to those at risk of severe disease from a respiratory pathogen. It is one of the four pillars of infectious disease response. Telling high risk patients to return once they have symptoms was a sure-fire way to increase the death count. Ivermectin, hydroxychloroquine and other treatments were demonized. Doctors prescribing them are being deregistered for saving lives, even today.

Remdesivir
Remdesivir is a highly toxic drug, particularly to kidney function. It is also highly profitable, earning Gilead US$4.2 billion in the first nine months of 2021 despite an October 2020 World Health Organization study showing “little to no effect on hospitalised COVID-19“. It continues to be promoted in covid treatment protocols, including in New Zealand.

Sedation Protocols
Nowhere have the lethal protocols of sedation, paralysis and high pressure ventilation been more headlined than the UK, where the documentary A Good Death? was filmed, drawing attention to the use of midazolam and morphine to kill vulnerable care home residents. These murders are highlighted by the case of Derek Dimmock, admitted to Royal Trinity Hospice in South London with severe gout and placed on an end-of-life protocol which killed him within days.
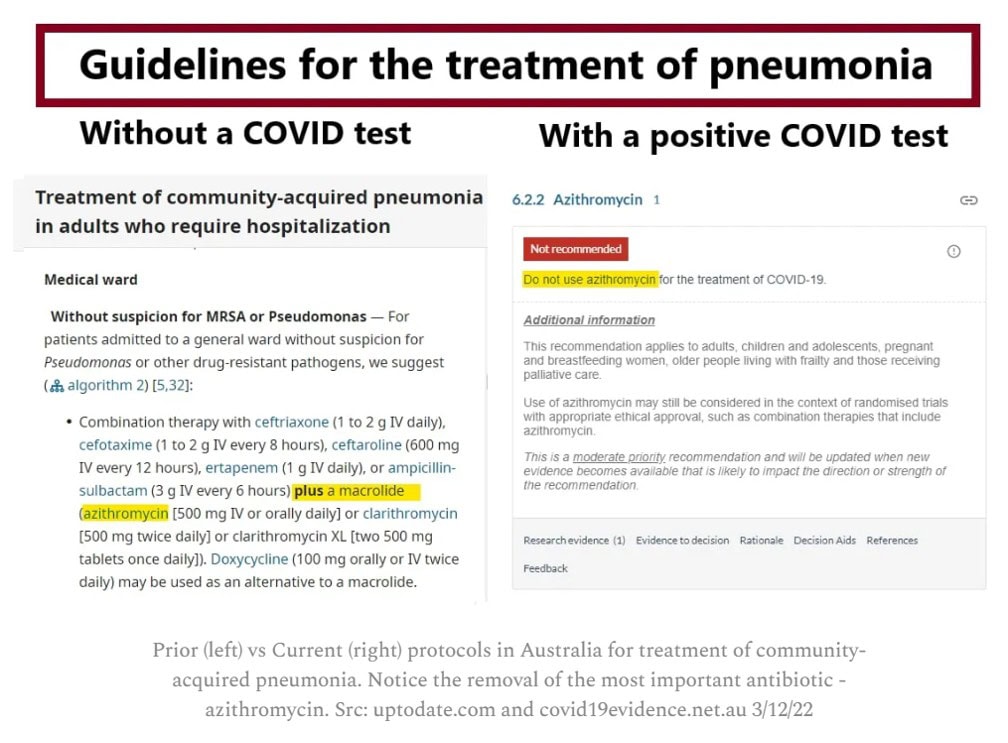
Antibiotic Denial
In 2008 Anthony Fauci published Predominant Role of Bacterial Pneumonia as a Cause of Death in Pandemic Influenza: Implications for Pandemic Influenza Preparedness in the Journal of Infectious Diseases. Inclusion of the antibiotic azithromycin in early treatment protocols for COVID-19 yielded the lowest mortality. Yet a leading cause of deaths in COVID-19 was secondary bacterial pneumonia, following the removal of antibiotics from treatment protocols.
Ongoing Pandemic Crimes
Despite the known relationship between healthy economies and healthy populations, western economic systems are being gutted. The cost of so-called pandemic preparedness is escalating with multi-billion dollar budgets. This will strip the capacity of services to address health issues of significance and intensify service strains. The corporate capture of health care was laid bare in Dr Bob Gill’s 2018 documentary, The Great NHS Heist.
Given the plethora of evidence it seems highly likely that the pandemic killing fields are a deliberate attack on humanity and society. With an incoming bird flu pandemic on our doorstep, New Zealanders must become aware of the threats being posed to our health in order to benefit corporate interests.
Once enough of us understand that harm is being used to generate profits and impose centralised control, then a move towards institutional reform focused on basic principles of public health can be restored. International efforts towards this are already underway such as the International Health Reform Panel and the REPPARE Research Project.
In his June 2026 expert witness testimony to the Brandenburg State Parliament Inquiry, world-renowned micribiologist Professor Sucharit Bhakdi gave this damning evidence on the extent of harms which have and are already taking place.
What Can We Do?
Every citizen has a moral duty to act in some small way to help end what Professor Bhakdi rightfully calls “the greatest medical crime in history“. NZDSOS have been relentless in our attempts to warn authorities and citizens alike. A shift in public perception is happening slowly. Those already aware of the crimes taking place must continue to speak up, dissent against nonsensical regulations and place as much political pressure on those in positions of authority and influence as possible.