Jodie Bruning on Ministerial Juggernauts and Vaccine Legislation

Powerful work by NZ researcher and academic Jodie Bruning adds to the canon of proof that the Kiwi segment of repeated ‘needles into every arm on the planet’ challenged our accepted norms of open democracy, responsible and accountable officialdom, and human rights.
The mildness of the actual illness NEVER justified any departure from traditional public health approaches to cold and flu-type viruses, and certainly not lockdowns of the healthy, illogical and traumatising masking, and social and economic devastation. Florid safety signals for the untested genetic ‘shot in the dark’ were already triggered overseas before our own rollout even started here, and have only increased with a trail of dead and devastatingly injured that the government and media are ignoring at best, and flailing desperately to hide at worst.
NZDSOS maintains that every single concern and fear we have voiced since the start is being clinically confirmed with consistent and reliable data, but officialdom has not responded and proceeds with its marketing of endless boosters, most damningly to the pregnant. This is surely criminal behaviour. Even the Justice Department tried – and failed – to talk human rights to the Prime Minister’s office, according to recently released documents.
Responses to determined OIA requests by brave souls like author Jodie Bruning, lawyer Sue Grey and others are triangulating just how much officials did know early on, which makes their relentless S&E narrative – still chanted like a stuporous drinking song – even shonkier and more damaging.
It seems increasingly apparent to many that the ‘health emergency’ of the last 3 years has been just a trojan horse for a last-ditch power grab, perhaps to drive humanity in an Orwellian direction before it can emancipate itself from the limitations (for most of us) of the arbitrary political and economic systems we are being held back by.
Jodie provides important pieces of the proof that democracy may be truly leaving the building unless we act firmly and fast. The fear induced by covid-19 has rendered many of us, including our officials and regulators, distracted and inattentive. Never have the safeguards provided by absolutes like the Bill Of Rights Act (BORA) and the codes of Nuremberg, Geneva, Helsinki and the UN been more proven in their original intent – a firewall against authoritarian and tyrannical leadership.
This article was first published at the Daily Telegraph.
Ministerial Juggernauts and Vaccine Legislation
JR Bruning 2023-05-16
The problem with secretly produced legislation.
We can now demonstrate how the over-riding COVID-19 goal for officials, from August 2020 onwards, was high vaccine coverage. The power and resources directed through New Zealand’s most powerful Ministries to support the ‘largest immunisation programme undertaken in New Zealand’ was further enabled by organisational structures with privileges that enabled them to sequester information – knowledge – from the public. The making of secondary legislation, the Ministerial Orders, and the justification for the production of the mandates was always secret.
What is also coming to light are the ways policy-making systems were decoupled from traditional legal, scientific and public health principles.
The result was a whole-of-government juggernaut, revolving around a single agenda, that was at such scale and pace it was impossible for officials and government employees to reject; that was so opaque it was almost impossible for the public to challenge. It could be observed in the secrecy of decision-making, and the capture of scientific information and, with it, the media and the judiciary.
This was not a public health operation which subscribed to traditional public health principles. It was top-down and authoritarian. It was techno-optimistic, with the vaccine purchase strategy led by Ministry of Business, Innovation and Employment, the Ministry of Foreign Affairs and Trade, and the Ministry of Health. We were solving the pandemic problem by subjecting every adult to the same treatment.
What minor official would contradict this power? The human and financial resources dedicated to vaccine uptake vastly exceeded resources which might contradict scientific or promotional claims, or challenge the global vaccination agenda.
It was ethically bankrupt because it prevented us from judging risk for healthy people. The State pressure on healthy pregnant women to receive the novel bioengineered genetic therapy was particularly immoral. New Zealand’s friendly propaganda urging pregnant women to get vaccinated, sharply contrasted with the harmful vaccine profile known by Pfizer and governments in early 2021. The vaccine could harm the mother, neonate, and newborn baby (through breastmilk).
New Zealand information, including the Immunisation Handbook (January 2022 edition), swept all pregnant women into an elevated risk category (despite referencing reviews that highlighted comorbidity risk). Although risk for pregnant women was stratified to multimorbidity and socio-economic status government officials failed to contrast absolute risk from vaccination alongside background risk by age and health status. In addition, officials relied on pharmacovigilance reports but largely ignored injury risk reported in the peer reviewed literature.
Any danger should have been judged by family doctors who best knew the patient was at risk because they had higher rates of previous preterm birth, stillbirth, neonatal death, and pre-existing medical conditions. Instead, mandates, distancing and propaganda directed families to vaccination, distorting the principle of informed consent.
Doctors traditionally do not give new drugs to pregnant women, because of uncertainty around harm. An older person who is harmed from a drug may only suffer for years, but neonatal harm can impair life quality for a lifetime. The novel bioengineered genetic therapy should have been accorded the same caution. Mothers were assured that the spike protein wouldn’t leave the injection site. But biodistribution studies were never done on where synthetic spike protein can end up in the body. Because the trials had not finished, Pfizer explicitly stated:
‘currently insufficient data to make conclusions about the safety of the vaccine in subpopulations such as children less than 16 years of age, pregnant and lactating individuals, and immunocompromised individuals.’
Developing fetuses are exquisitely sensitive to toxic insults, even at parts per billion or trillion. Adverse effects may be unknown or risk downplayed. The lessons from the hormone disrupting drug Diethylstilbestrol (DES), and the morning sickness ‘miracle cure’ Thalidomide include the difficulty of victims in seeking redress; and that even properly tested and registered medications can turn out to be disasters. In the case of DES, the harm was to the next generation of daughters. State funding for researching environmental harms is minimal, but disaster examples are legion: asbestos, Agent Orange, DDT, lead, mercury, pesticides including of course glyphosate, fluoride and, of course, ambient communication microwaves and EMFs. There are few scientists with expertise and secure core funding who might speak up.
The laws developed to support the ‘jab’ campaign, made it almost impossible for the public to contradict through judicial review, because the laws revolved around chasing infection, rather than protection of health and preventing hospitalisation and disease in the most vulnerable.
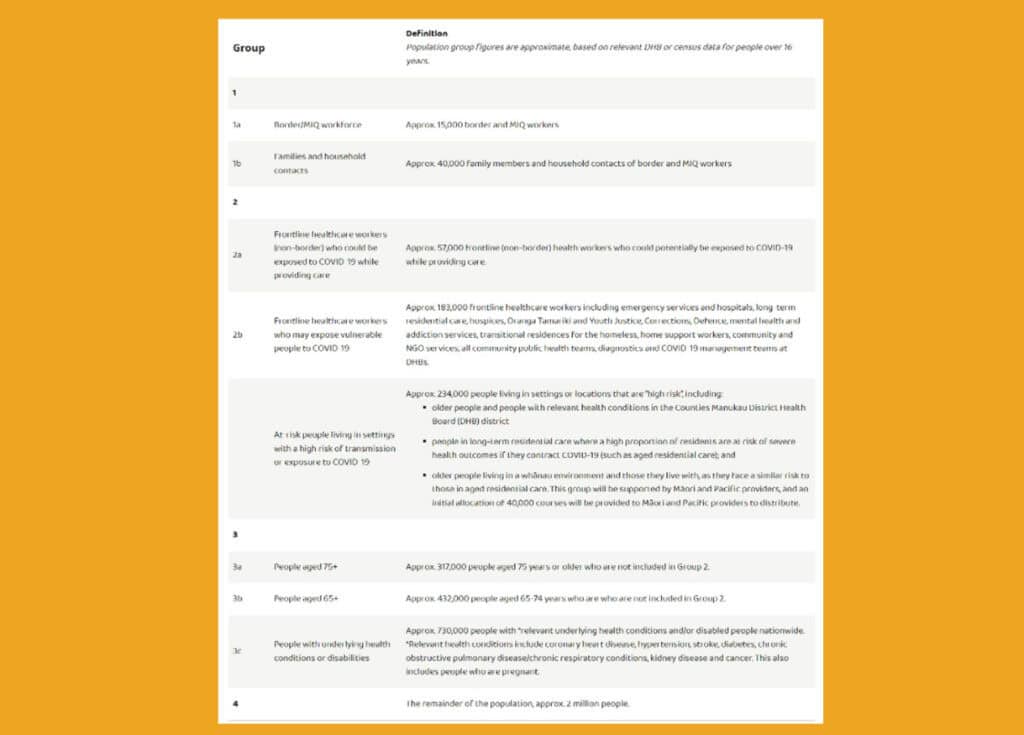
The public unease at the rollout plan, first understood as the ‘sequencing framework’ contrasts sharply with government messaging that hard-line tactics were justified. Most unease surrounded the mandatory deployment of the experimental medication, a novel mRNA, a novel bioengineered genetic therapy (coded BNT162b2) that, contrary to older, traditional vaccines, instructs the body to reproduce an (synthetic) S-protein, a copy of the virus spike protein. The scientific literature has recognised the harmful potential of the spike protein for over a decade.
The departure away from ordinary democratic processes that promote trust, the decoupling from these principles, has been extraordinary, over the COVID-19 era. Possibly the strangest decoupling, was the act by the Attorney-General, list MP David Parker, to remove obligations that Ministers had to abide by the Health Act when making Orders.
Important protections & principles jettisoned
Parker achieved this via the secret, overnight COVID-19 Public Health Response Bill of May 13, 2021.The COVID-19 Public Health Response Act (the COVID-19 Act) ensured that Orders produced under section 11were not required to adhere to traditional obligations and principles required under the Health Act 1956. This was done by deliberately removing the authority of the Health Act relating to Orders (and therefore mandates).
13 (1) A section 11 order may not be held invalid just because—
(a) it is, or authorises any act or omission that is, inconsistent with the Health Act 1956 or any other enactment relevant to the subject matter of the order; or
(b) it confers any discretion on, or allows any matter to be determined, approved, or exempted by any person
This scythed off a requirement to consider individual health, particularly the impact on young people children and pregnant women. First, the obligation to improve, promote and protect public health would not be required as a mandatory consideration. Judicial review of actions taken using the power of the Orders simply had to confirm the fulfilment of the purpose of the overnight COVID-19 Act. Secondly, the highly relevant overarching principles, (see Part 3A, Subpart 1) required to be considered by officials when managing an infectious disease, where not required to be mandatorily considered, either.
That these two rather obvious considerations could be jettisoned, so lightly and so effortlessly, by overnight legislation, is my pick for the single most important policy and legislative failure.
Instead, the key COVID-19 legislation gave power to Ministers and officials to take action that would prevent, and limit the risk of, the outbreak or spread of COVID-19; and action that would avoid, mitigate, or remedy the actual or potential adverse effects of the COVID-19 outbreak.
‘Adverse effect’ was never defined to include adverse effects from interventions as time progressed, particularly for people who were not at risk of hospitalisation and death. There was no requirement to associate an outbreak with severe death and/or disease, because this wasn’t required by the World Health Organisation under its revised definition of pandemic. The infectious agent didn’t have to send people to hospital for these laws to be made. The laws revolved around officials dealing with a COVID-19 outbreak.
Relatedly, no distinction was made in the legislation between Sars-CoV-2 outbreaks of infectivity as defined by the grossly oversensitive PCR test, and the disease itself, COVID-19, of which, in March 2020, most people were not at risk. Additionally, its much more modest fatality rate was already trickling into the literature by then.
Astonishingly out of fashion perhaps, but in drug development, safety is always the primary consideration, before efficacy. No matter how effective a drug is, it has to be safe. We can’t always depend on the drug producer, which is why it is important to methodologically review the literature as an emergency event progresses, including looking at different study designs, and triangulate the evidence. It’s not enough to rely on claims of the manufacturer or pull together reports that have no methodological basis and invite accusations of cherry-picking. But there was no stopping point, when injury and death from the novel bioengineered genetic therapy would signal that the injection campaign should cease. No such considerations were in place in the legislation – particularly, in the vaccinations legislation of then Minister Hipkins.
This meant inevitably that applicants for judicial review would never get a judgement that government actions were not protecting health, that the response did not have to be proportionate and consider the individual, which were obligations in the Health Act. The over-riding legislation never discerned that people had stratified risk to respiratory viruses, just like they always had been. Parker and Hipkins put in place blunt instruments.
But the legislation gave officials and Ministers extraordinary powers.
Ministerial priviledge and secrecy
Government policy and law was constructed swiftly and secretly through meetings of the Executive Council. As the highest formal instrument of government, the Executive Council sets in play Orders in Council, which are then sent to the Parliamentary Counsel Office for drafting. Theoretically Cabinet must approve all matters for consideration by the Executive Council.
But every bit of this pathway was carried out in secret. What is rather eye-opening, as the Cabinet Manual notes (2017, and the newer 2023 edition), is that the Executive Council merely require only two Ministers in attendance to constitute a quorum, plus the presiding officer. Prior to the COVID-19 era, Orders which would impact the entire population had never been produced.
The Ministers’ belief that each new Order was justified, never had to be publicly demonstrated. No supporting information that would provide a background had to be supplied, such as a regulatory impact statement. It is evident that impartial, procedural reviews were never undertaken, including of the scientific literature that might reveal how the synthetic messenger-RNA injections, a novel bioengineered genetic therapy, impacted the human body. Globally, scientists were working hard to draw attention to all aspects of risk and treatment, throughout the pandemic.
 But because of the way our legislation was constructed, research which might triangulate Pfizers’ claims of efficacy and safety was out of scope. Market authorisation had been based on company data only, and New Zealand’s overriding legislation did not require broad-based reviews that shed light on the published scientific knowledge concerning the safety and efficacy of the synthetic messenger-RNA injections.
But because of the way our legislation was constructed, research which might triangulate Pfizers’ claims of efficacy and safety was out of scope. Market authorisation had been based on company data only, and New Zealand’s overriding legislation did not require broad-based reviews that shed light on the published scientific knowledge concerning the safety and efficacy of the synthetic messenger-RNA injections.
This dark space – the Cabinet discussions we can’t see, the company data we are denied – enabled the weaponization of Ministerial Orders (which produced the mandates) to an extraordinary degree. The public cannot even access the dates Orders were instructed to be produced, such is the extent of secrecy.
At the same time the corporations who entered into vaccine supply contracts have secured a privilege the public could not dream of. From early discussions with vaccine lobby groups, to contract negotiation and signing, to the Pfizer/BioNTech safety and efficacy data, and then the unfortunate post-marketing results, it’s all kept secret. Even the financial losses of stale vaccines remain hidden.
The secret post-marketing report.
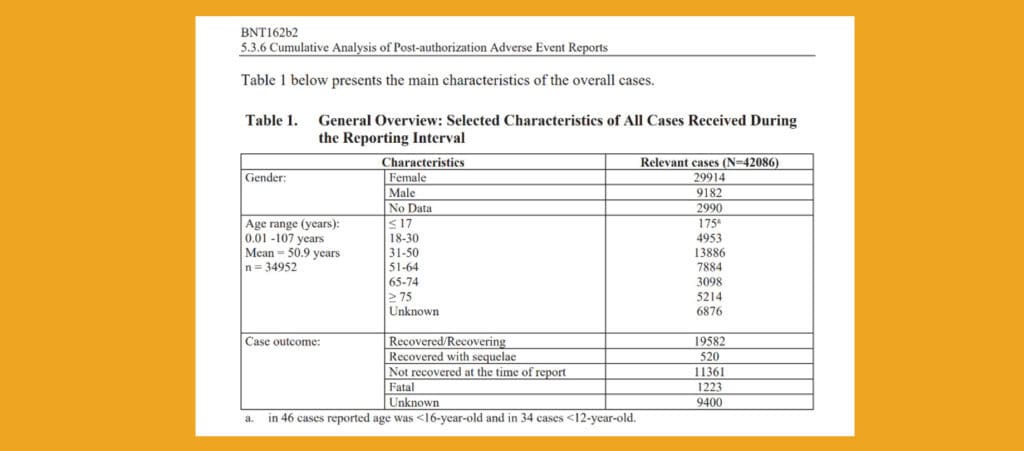
By traditional standards, Pfizer’s February 2021 post-marketing report which detailed extensive adverse events, should have triggered a safety review. These adverse event reports had to be supplied to Medsafe within five working days of being produced. It has been difficult to establish when this information drop might have arrived, with New Zealand officials claiming that the FDA document was produced for only a specific legal purpose. Officials seem to be skirting around the issue.
This inconvenient report may have arrived at about the same time that the March 10, 2021 Rollout Plan was released. The plan lodged an expectation that civil society would be ‘vaccinated’. Clearly, the government intended for the entire population to be injected with strange new technology, evidenced by signing an initial advance purchase agreement for 8.5 million doses.
Over the next year, the production of Orders was always consistent with this expectation and timeline.
Officials must not shy from briefing Ministers on controversial matters. The Department of Prime Minister and Cabinet (DPMC), should have been briefed of the newly understood and alarming harm profile revealed in the February 28 2021 post-marketing report, and this information should have been held with the DPMC.
But they refused to answer my request for memos or advice directly relating to this data, noting that, of course, the mandates came from decisions made by the Executive Council. This information was relevant to decisions to widen mandates.
My March 2023 OIA request to the Ministry of Health sought to identify discussions relating to the post-marketing data, as I recognised the Ministry have been reluctant to publish this data.
Strangely, the Ministry of Health flicked part [a] of the request to Te Whatu Ora, which wasn’t invented at the time of the request.
“Please supply urgently, between 27 February 2021 and 9 March 2021 the following information:
[a] All discussions via WhatsApp, Signal, Messenger, private email, Parliamentary or
political party email by officials, including Ministers and the Director General of Health
discussing Pfizer, BioNTech, the post-marketing report, FDA, deaths and adverse events.
This was rejected by Te Whatu Ora. Apparently, my request for ‘reports, releases, memos and advice’ between 27 February 2021 and 9 March 2021 would ‘require substantial collation due to the hundreds of employees and potentially thousands of Messages’.
The second part of this request (H2023021708) concerned access to
[b]All reports, releases, memos, advice discussing and/or reviewing the implications of, contents, evidence in the post-marketing report supplied as a requirement in the Gazette conditions, and taking all steps to reasonably consider the harm profile to the population who were not at risk of hospitalisation or death from COVID-19 (required by Health Act, Part3A, s.92, Overarching Principles). This includes the risk to pregnant women, young people and children.
The Ministry of Health rejected my request on the following grounds:
- section 9(2)(b)(ii) where its release would likely unreasonably prejudice the commercial position of the person who supplied the information.
- section 18(f) as the information requested cannot be made available without substantial collation or research.
- section 9(2)(a) to protect the privacy of natural persons
Then I considered that an understanding of the department and dates might be reasonable. But the response to that OIA request (HR2023022884) confirmed that the public are not permitted to know who was responsible for managing this up to the February 28, 2021 information drop. This was refused as it might lead to improper pressure or harassment. Nor are we permitted know on what dates the post-marketing information arrived. I did not specifically ask for adverse events to February 28, yet I suspect that Medsafe Manager Chris James and the Ministry of Health understood very well that “post-marketing report” concerned the same information as was in the FDA’s Cumulative Analysis of Post-authorization Adverse Event Reports.
So, it seems we cannot know the information that was produced, nor the dates Medsafe received it. We cannot risk the reputation of the manufacturer, and strangely, official staff privacy needs to be protected.
The dates when Ministers decided to produce the next Order are secret too.
The extent to which we are not permitted to understand the information used by responsible Ministers to justify the Orders, was highlighted when I attempted to understand the dates when Orders were first instructed to be made. By understanding the dates, I could perhaps establish what information was received by then Minister of COVID-19 Response, Chris Hipkins – now Prime Minister – to justify the increasing mandates.
I made Official Information Act requests to the Parliamentary Counsel Office, the DPMC and the Ministry of Health. I wanted, simply, to understand the date instructions were made, to firstly (a) make editorial changes to all reprints of the COVID-19 Public Health Response (Vaccinations) Order 2021 from 14 July 2021 onwards; and secondly (b) commence drafting of: COVID-19 Response (Vaccinations) Legislation Bill 2021.
I didn’t ask for the contents which of course would be secret, just the dates. But once again the DPMC flicked my request to the Ministry of Health, even though, of course, the Order decisions come out of Executive Council meetings.
Therefore when I expressed surprise that the information would have been sent through Ministers and/or Cabinet officials, the DPMC Ministerial Co-ordinator acknowledged that:
The request was transferred, following consultation with the Ministry of Health, as it is more closely connected to their work and functions. The transfer does not mean the information was not sent through Ministers or Cabinet officials. A response will be provided by the Ministry of Health which will provide details of this work.
Even though the Ministry of Health administers both the COVID-19 Public Health Response (Vaccinations) Order 2021 and the COVID-19 Response (Vaccinations) Legislation Act 2021 this information would have been held by the DPMC. Remember, the Executive Council – the council which comprises all Ministers of the Crown – has a principal function of advising the Governor-General to make Orders in Council.
The instructions are then passed to the Parliamentary Counsel Office (PCO) who are responsible for drafting most of the documents for the Executive Council. I was aware that the PCO was not subject to the Official Information Act but I wondered if the date of each instruction would be hidden by confidentiality rules. The PCO responded with:
This isn’t something we can help you with, however. Drafting instructions, and related communications between the instructor and PCO, are confidential and subject to legal professional privilege (see section 131 of the Legislation Act 2019).
The Ministry of Health then responded to confirm that the dates were subject to legal and professional privilege. Chief Legal Advisor Phil Knipe noted that he did consider
‘the countervailing public interest in releasing these drafting instructions and consider that it does not outweigh the need to withhold at this time.
The question is begged, on what basis? Knipe directed me to this page, which contains no information in relation to the Orders requiring affected persons to be injected, and then that the public carry COVID-19 Vaccination Certificates (CVCs). Information specifically concerning mandate Orders was not on this page.
Such is the extent of secrecy. However, a law that required everybody to submit to a medical treatment should be underpinned by impeccable reasoning. The decision to make that law, must be understood at that time to be reasonable and fair-minded, and withstand legal scrutiny.
But we are not permitted to be privy to that information.
By the time the rollouts and accompanying laws were being made, there was substantial intelligence available that the emergency event had been overstated, that most of the population were not at risk from COVID-19. The chosen medical treatment, a novel genetic therapy that instructed the body to reproduce an engineered spike protein, was only one small element of the novel coronavirus. The technology was never designed for, nor efficacy based on, prevention of transmission.
But the Director-General, Minister for Health & Minister for COVID-19 (-) should have known.
Yet by mid-2021 Minister for COVID-19 Chris Hipkins, should have been shown the devastating post-marketing study that revealed unexpectedly high death and injury rates, including for pregnant women and neonates.
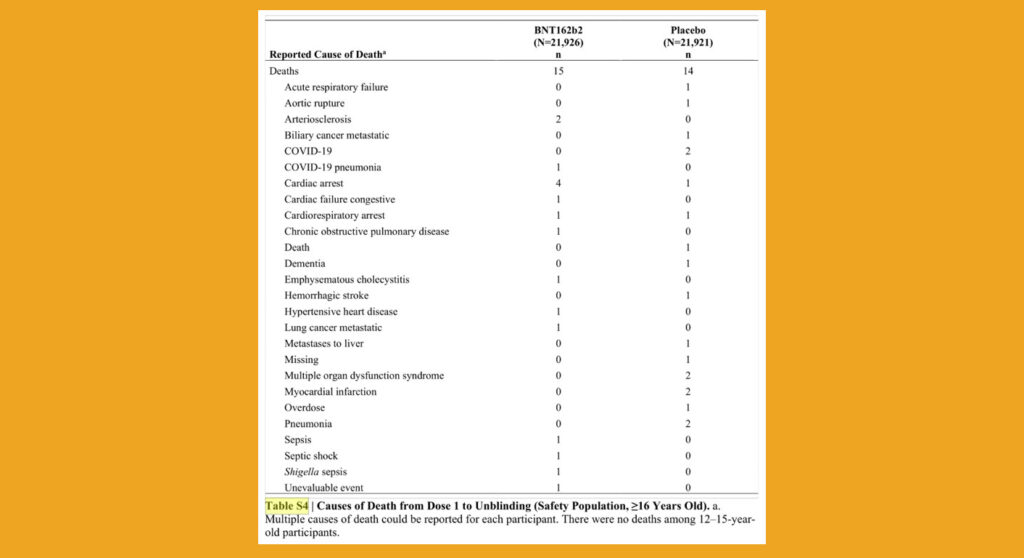
Governments should have had early (pre-publication) access to Pfizer’s 6-month trial data that revealed a higher death rate in the vaccine group than the placebo group, long before the data was formally published for public viewing.
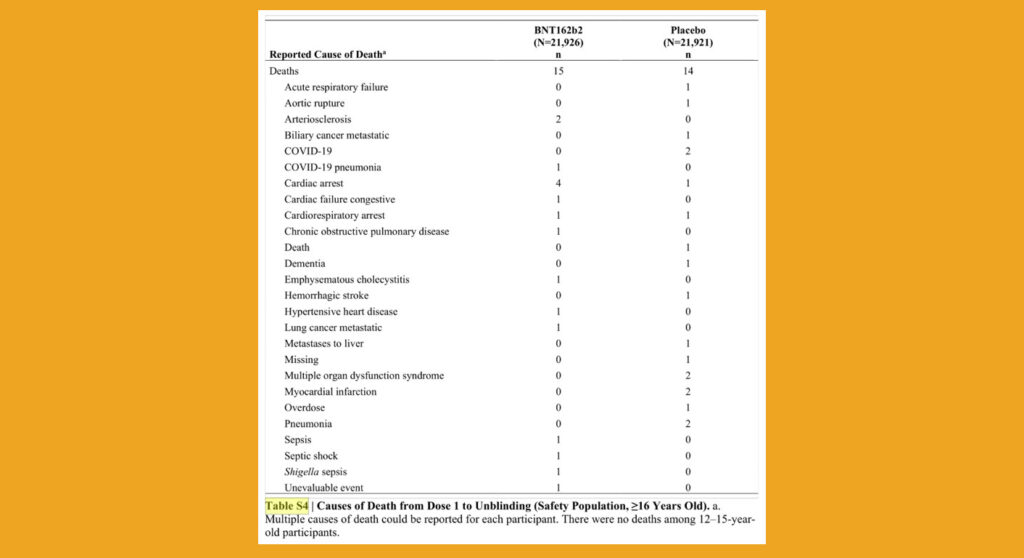
Governments should have had early (pre-publication) access to Pfizer’s 6-month trial data that revealed a higher death rate in the vaccine group than the placebo group, long before the data was formally published for public viewing.
Why should Hipkins have been directly shown this information? Because he was putting in place law demanding the public were injected. Laws demanding that pregnant women must be vaccinated to work, even though officials recognised that trials in pregnancy had not been completed and that pregnant women should clearly be informed of risks. Officials had an obligation to show him contradictory information.
As I have demonstrated, I’ve been unsuccessful in attempting to access any reviews or analysis of the disruptive implications for official decision-makers after New Zealand received our version of the FDA post-marketing report. I now consider it was buried.
There were no rolling reviews of the changing science relating to safety and efficacy. I asked Pharmac and spent enough time chasing the Ministry of Health to establish if there were methodological reviews of the changing scientific information. They’re not there.
Civil society would expect, logically, that the massive post-marketing information dump from Pfizer to the FDA would have been in the form of a single report to New Zealand’s Medsafe, given Pfizer’s contractual obligations to update safety information as it became available. We can’t know the truth because the barriers to us knowing are mighty.
The courts agree generally that limits such as mandates must serve a sufficiently important objective or purpose that warrants overriding a protected right or freedom, and that the means chosen to achieve the objective must be proportionate. With regards to the latter, the means chosen must be rationally connected to the objective, there must be minimal impairment, and the effect must be proportionate. The benefits achieved must not be outweighed by the significance of the limitation of the right.
This, the public would think, hinges on information. The provision of science.
But what remains obscured is the purpose and scope that gives Ministers and officials their powers, who then set the priorities – in this case, chasing after a quickly mutating respiratory virus, using an unproven highly risky biotech gene platform.
Yes, officials must not be biased, and must consider controversial information. Indeed,
‘An authority may unlawfully abdicate its statutory function by refusing or failing to act. A public body must not renounce its decision-making responsibility, nor preclude itself from inquiring into matters relevant to its inquiry.’ [Constitutional and Administrative Law in New Zealand, 4th Ed., P.A Joseph, 23.2.3, p.972]
Various factors do not portend well for the next emergency event, namely: the non-disclosures, and the obfuscation of unfavourable information that could contradict whole of government messaging, Because what we have seen over COVID-19 is an absolute failure of the Government to report honestly on the epidemiological evidence – namely who was most – and least – at risk from COVID-19, and why the experimental mRNA technology was unlikely to support the health of the most at-risk.
While the power to release Orders was amplified, the secrecy remained. To quote sociologist Samantha Crompvoets:
Power and knowledge, or rather the concealment of knowledge – secrecy – are two significant predictors of misconduct that can be seen in a number of institutional contexts.
But, I consider that by this time, officials were already numb, blandly avoiding inconvenient facts, including the absence of data on pregnant women, the likelihood it might not work on multimorbid populations, the absence of genotoxicity and carcinogenicity studies, and the reality that safety and efficacy was based only on limited symptoms one week after injection.
With the prevailing organisational structure (including legislation, policies and formal and informal power relations) in place, when the government did receive bad news, there was no obligation to disclose it. Complete obfuscation remains, around when the highly alarming and controversial post-marketing report/s were supplied to the secret people who were responsible for receiving this secret data.
For several years the New Zealand public have squabbled over informed consent, the legitimacy of mandates and whether the right to refuse medical treatment could be justified – in the courts, on social media, in families, churches and workplaces.
The upending of these supposedly ethical absolutes was enabled by Cabinet processes which enabled elite groups to act secretly, with little oversight and no accountability. This has been enhanced by a wizardly green curtain of scientific complexity, which often might have been simplified by following Health Act principles, and medical ethics. Crompvoets informs us further:
The more elite, secretive and cloistered a group is, the higher the chance of deviation, and the concealment of that deviation. This is exacerbated when the group or subgroups hold specialist skills that are not well understood by those outside of the organisation, and are revered or despised.
It’s not about the culture, it’s about the rules that let the players play the game. And over COVID-19, while knowledge was changing on a weekly basis, the rules were structured by the players to supercharge the production of laws outside public processes, while maintaining secrecy.
What lockdowns, what surveillance and what injections will be imposed on the New Zealand public, in the next emergency?









The NZ public in total must be made aware of all this and those responsible for the implementation of this scam / travesty of rights must be held to account and not allowed to ride off into the sunset unpunished.
Excellent article.
GOD bless you and all the people putting in so much effort into trying to expose what really went on.
Thankyou for another brilliant detailed expert analysis of the extraordinary process trying to obtain information about the timing, scientific evidence and rationale used by the government, to impose COVID mRNA biogenetically engineered Vaccines and coercive Mandates upon the people of New Zealand. The secrecy and obfuscation is distressing plus the fact that politicians in all parties seemed to be seduced and held under the thrall of this technological medical science authoritarian transnational corporate power.
Truth always wins, in the end…
The amount of compounding lies we have and still are being told by our ‘dishonest nz representatives’ is unprecedented. The simple fact that they harp on about misinformation and disinformation being public enemy number one whilst themselves have continued to contradict almost everything they say, blatantly lying to the nz public should be enough for any halfwit to start asking questions as opposed to continue supporting a complete unethical and immoral government narrative? How can a heathy debate not happen anymore, especially when it relates to the bodily autonomy, health and well being of every single kiwi citizen, that in my opinion is complete ludicrously, irresponsible and immoral behaviour which cannot and should not be ignored, especially when it relates to the ‘best’ interests of every kiwi.
Enough is enough and know is the time for all kiwi’s to stand as one, united in bringing an end to secrecy of the information that either directly or indirectly impacts our heath and well being, creating ‘true’ informed consent measures and start bringing the culprits of the largest poison pushing campaign in history. Unfortunately that is but only one piece of the ‘corruption’ pie that kiwis have been force fed and is only what is visible to the human eye, the more covert issues are of grave concern also, such as poison being put in our food, water, air and the issue of geo-engineering and the manipulation of our weather that have and are causing detrimental long lasting effects on the good kiwi people are issues that need a public forum in which to be debated and steered into the direction of the kiwi public’s best interests, not those who’s pockets are lined with gold for manipulating policies in secrecy that clearly do not promote the best health outcomes for us kiwis but rather fill their pockets with more gold whilst the detrimental effects will continue and flow on to future generations. What happened to logic? Red flags have been waving in all of our faces on a daily basis for over 3 years now and yet we still have a great disproportionate amount of kiwis ignorantly accepting the lies we are fed from a corrupted government that are nothing more than puppets for the elite, bidding on their behalf with not a single concern for kiwis health.
The who, wec, un and other corrupt global institutions need to be dismantled and dissolved asap, with every single member and financial contributor being investigated in regard to their global dealings, from every email, text and other forms of communication between them and government departments. I’m sure that would show an unprecedented and unparalleled amount of misinformation and disinformation that would shock the global public to the core! The good news is it would also lead to an overdue amount of ‘justice’ for the people who have lost their lives and have been left with debilitating health issues caused from these egotistical, egomaniacal greedy power hungry monsters! Then and only then the good honest decent global citizens can go about rebuilding a world where the health of every single person comes before profit and install Nuremberg 2.0 global policies to ensure these monsters will never ever again have the power to override the ‘people’s’ policies.
One only needs to have heard (and remembered) JFK’s thundering speech about the abhorrence of ‘secrecy in govt’) to recognize from its beginning the threat to human life this jab had to be. This, together with the shady characters behind it + the unscientific notion that ‘one size fits all’, was for me enough to step back from even considering it. Since then I’ve been horrified every day seeing the continuous mayhem of people collapsing far and wide, and it left me thirsting for justice. I think it won’t be until the present crop of politicians + judiciary becomes a minority, that the winds of change will be strong enough to blow away the cobwebs of ill will, doubt, treachery, and the war on truth in general. Until then it is our duty to keep alive this one sentence: “Lest we forget”.