Safety Monitoring and Adverse Effects

The following is about the Safety Monitoring and Adverse Effects of medicines. One of the fundamental ethical principles of the practice of medicine is First, Do No Harm.
Background
This article refers specifically to the Pfizer vaccine (Comirnaty) which has been available in New Zealand since February 2021.
Comirnaty has been rapidly produced to combat Covid-19. It has been called a ‘vaccine’ although it is unlike any previous vaccine used in New Zealand. It uses new types of technology – mRNA (genetic material – messenger ribonucleic acid) encased in lipid nanoparticles. mRNA technology has been around for a number of years but has not been used on a wide scale in healthy populations before. The lipid nanoparticles (ALC-0315 and ALC-0159) are new as well.
This ‘vaccine’ could also be called a gene therapy, as it is using genetic material to alter the way the body works. Most traditional vaccines use a part or all of the organism to be protected against, in their manufacture. This vaccine, instead, allows for the injection of synthetic genetic material. These genetic instructions cause some of the body’s cells to become manufacturing plants for part of the Coronavirus – the spike protein to be specific. The idea being that the immune system will recognise this spike protein as foreign and will then create a defence against it.
The Pfizer vaccine available in NZ was developed during 2020, and a study was published on 31 Dec 2020 in the New England Journal of Medicine (NEJM) (1) that detailed the interim results of the Pfizer/BioNTech clinical trial. This trial (which is due to be completed in May 2023 (2) ) is studying approximately 44,000 participants split into two groups – half initially given the vaccine, half initially given a placebo. Data collected in the three months between July and October 2020 was analysed. There was a median of two months follow up for the participants when the study was published. The outcomes of 170 of the 44,000 participants allowed Pfizer to determine that the vaccine was 95% effective. Eight participants in the vaccine group and 162 participants in the placebo group were diagnosed with Covid 19. The relative risk reduction was therefore 95%.
Provisional Approval
On the basis of these interim results, Medsafe gave provisional approval to the Pfizer vaccine in February 2021. The provisional approval came with 58 conditions (3). Some of these 58 conditions related to possible safety concerns. When contacted to ask what the outcome of the 58 conditions were, Medsafe replied: “The information submitted to Medsafe by Pfizer to address the conditions of the provisional consent for Comirnaty is considered commercially sensitive, and is therefore withheld under s9(2)(b)(ii) of the Official Information Act 1981”.
The initial provisional approval lasted nine months until 2 November 2021. On 28 October 2021 the provisional approval was renewed for a further two years with only eight conditions (4). It was not given full approval.
This is all significant because this is a new type of medication. It has not been used in healthy humans before. The clinical trials are not yet completed. Medsafe gave it provisional approval on the basis of very limited data, and has only renewed its provisional approval rather than granting it full approval. At the very least the Precautionary Principle should apply, i.e. it should be considered that it could be dangerous until it is proven safe, rather than the other way round – assuming it is safe until proven harmful.
Is it ethical to be administering it to everyone, particularly pregnant women, children and young people?
Just because a medicine has been given to millions of people does not make it safe. We are repeatedly being told that if there were problems, it would be obvious by now. Most vaccines and new medications take at least five, if not up to ten years or more, to develop and go through the appropriate safety testing. This vaccine might have large volumes of data but there IS NOT and CANNOT POSSIBLY BE long-term data. The first doses in the trial were administered in July 2020, less than 18 months ago.
Diethylstilboestrol was considered to be safe for pregnant women and was prescribed in the 1940s to 1960s to prevent miscarriage. It wasn’t until years or decades later when the children reached adulthood that problems were found – including genital tract cancers and fertility issues. Adverse effects from this medication are still being experienced by sons and daughters of exposed mothers today. (5)
Two of the eight conditions of the continued provisional approval require Pfizer to provide safety reports – a monthly one and a periodic update in line with the European Medicines Agency. It is not clear if these safety reports will be able to be viewed by the public. This means safety is still being assessed. What happens if it is determined that it is not safe, or is the outcome of the safety testing a foregone conclusion?
A significant problem with the ongoing reporting from the trial is that a large number of the placebo group have been given a vaccine. The placebo, or control group, is now significantly smaller than it was, and the final data will be much less robust.
Safety in Teenagers
The latest Medsafe Comirnaty data sheet (6) (a document used by New Zealand doctors wanting a summary of important information about a medication) says for adolescents 12-15 years of age, the safety data comes from 1,308 participants (only 660 given the vaccine) followed for at least two months. It also states: “The safety evaluation in Study C4591001 is ongoing.” What if this ongoing evaluation proves that it is not safe for teenagers? Is 660 people and two months of data enough information to guarantee safety for all teenagers?
Safety in Younger Children
With regards to 5-11 year olds, a new formulation of the Pfizer vaccine Comirnaty has recently been approved by Medsafe for use in NZ. Study C4591007, which includes 5-11 year old children, only started in March 2021 and is not expected to be completed until May 2026. (7)
The Medsafe data sheet for the new formulation for younger children (8) shows that only 1,518 children aged 5-11 years have been included in the study for safety and only two months of follow up for 1,444 of them has been collected to date.
This data sheet also says that this vaccine has not been studied in conjunction with other vaccines or medicines, in immunocompromised children, or for the possibility of causing cancer or damage to genes. It also advises that the duration of protection is unknown.
This is some of what Pfizer has to say about safety in this age group in another document (9): “The number of participants in the current clinical development program is too small to detect any potential risks of myocarditis associated with vaccination. Long-term safety of COVID-19 vaccine in participants 5 to <12 years of age will be studied in 5 post-authorization safety studies, including a 5-year follow-up study to evaluate long term sequelae of post-vaccination myocarditis/pericarditis.”
Surely most parents would want this information to be available prior to agreeing to this vaccine.
Post Market Surveillance
When a medicine is released, either early or after an appropriate length of study, it is followed up with post-marketing surveillance. This is a passive system and relies on the voluntary reporting of adverse effects to the regulatory agencies.
On the Medsafe website it states that only about 5% of adverse events get reported (10). This is consistent with international expectations of between 1 and 10 % of adverse events being reported.
Why would that be?
For an adverse event to be reported, several things need to happen:
- The person needs to consider the symptoms to be related to the vaccine
- The person needs to seek medical attention
- The doctor needs to consider the condition may be related to the vaccine
- The doctor needs to know there is a reporting system, that he or she should be reporting every new condition, and know how to access the system
- The doctor needs to have the time to report it
- The doctor needs to have the correct information to upload
- The doctor needs not to be censored with regards to what can and can’t be reported
- The system needs to be working and easy to use
A problem with any one of those steps means that a report might not get made. For example, the NZ Medsafe’s CARM online reporting system is laborious, time-consuming and isn’t always functional.
Or, another example – the person needs to consider the symptoms might be related to the vaccine and the doctor needs to do the same. The public and doctors in New Zealand have been given a list of fairly benign expected adverse events – sore arm, headache, fever, nausea, fatigue, and told to expect the symptoms to last for, at most, a few days (11).
Doctors have not been told that heart attacks, strokes, new neurological conditions, seizures, adverse pregnancy outcomes or altered menstruation could be side effects of this vaccine. In fact doctors have expressly been told that there are no safety concerns with this product in pregnancy (12), no risk of blood clots with the vaccine (13) and no connection between menstrual disorders or unexpected vaginal bleeding and the vaccine (14). The only serious adverse event, that may potentially follow the Pfizer injection, that doctors have been warned about, is myocarditis and that is supposedly very rare (15).
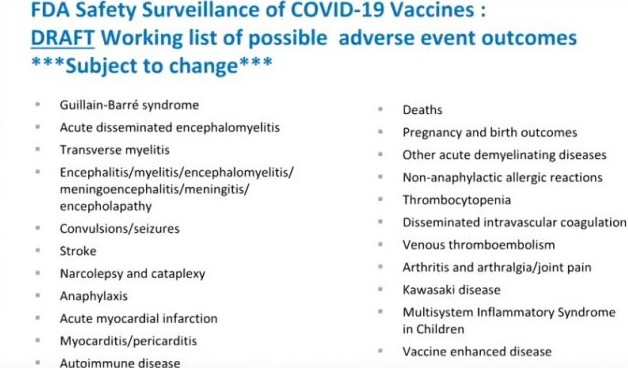
This is in sharp contrast to what Pfizer knew it might expect to see. At an ACIP (Advisory Committee on Immunisation Practices) meeting in October 2020, there was a presentation about Monitoring Vaccines for Safety and Effectiveness (16). Slide 16 of this presentation details a long “working list of possible adverse event outcomes” for Covid 19 vaccines. This list includes death, Guillain Barre syndrome, seizures, heart attack, stroke, vaccine-enhanced disease, auto-immune disease, pregnancy and birth outcomes along with many other conditions.
Doctors, like the public of NZ, have been told this vaccine is ‘safe and effective’ and have not been advised to consider any of these as possible adverse events following Covid vaccination.
One final word about post-marketing surveillance. For it to be effective, someone needs to analyse the information once reports have been made.
Safety Monitoring and Adverse Event Reporting in New Zealand
NZDSOS has communicated with a significant number of people who are advising that their possible adverse reactions have been fobbed off by medical staff as being unrelated to the vaccine. They have been told (sometimes repeatedly) that it is just a coincidence or that they are anxious. This is confirmed by health professionals working both in hospitals and General Practice – a lot of potential reactions are not being reported.
The role of health professionals in adverse event monitoring is to REPORT EVERYTHING that occurs following vaccination, not decide whether it is related or not. That is the role of CARM and/or Medsafe who are analysing the whole data set.
The public won’t have confidence in the system if they, or their concerns, are repeatedly dismissed. Doctors are taught to LISTEN to the patient, as that is where the essence of the diagnosis is – in the history. Why would doctors suddenly not be listening to their patients and be dismissing them when they say “I was perfectly fine until I had this vaccine”, or, “my symptoms started a few days after the vaccine”?
Imagine if 500 doctors around the country are seeing the same peculiar event and each is dismissing it and not reporting it. One is an anecdote, but together 500 might be significant.
How long should this reporting continue? If proper safety monitoring was being done, this would continue for ever more. New medical events in vaccinated individuals should all be reported – at least for the next 10 years but ideally much longer than that. It is going to be difficult to know what the ‘background rate’ is though, as there will only be a small control, or unvaccinated, group for comparison.
Some places overseas have reported that the vast majority of adverse effects or deaths are due to a small number of batches of the vaccine. It would be interesting to know if that was the case here.
Adverse Events
Worldwide databases collecting the adverse event information have had vastly increased numbers of events reported in the past year – the VAERS database in America, the Yellow Card system in the UK and the European database, Eudravigilance.
In New Zealand we have CARM, based out of Otago University. Normally this system gets 3-5 thousand adverse event reports for ALL medicines over a 12 month period. In the 10 mths of 2021 from the start of the vaccine rollout, they received over 45,000 reports just for the Pfizer vaccine. This included over 2,000 reports of serious events and 133 deaths. (17) If only 5% of reactions are reported, these numbers could be 20 times higher.
Now, not all of these will be due to the vaccine – some will have occurred coincidentally shortly after vaccination. But how is this causality or non-causality being determined? What rigorous or robust processes are actually in place to figure this out? If CARM normally assesses 5,000 reports and now there are over 45,000, that is an over nine-fold increase. How are they going to do that much extra work? Have they employed nine times as many extra staff?
On the Medsafe website until mid December 2021 it stated: “Medsafe has not yet finalised all of the methods that we will use to monitor COVID-19 vaccine safety.” (18) Did that mean they spent most of 2021 trying to figure out what to do with all the data? This webpage has now changed (19) to provide more information about safety monitoring including the introduction of more active safety monitoring with Post Vaccine Symptom Check.
Deaths
With regards to the 133 deaths that have been reported to CARM as of 31st December 2021, were post-mortems done in all these cases? Were they done in any of the cases? It is well known that NZ has a shortage of pathologists and it is difficult to get a post-mortem done in normal times.
Fifty-four of the 133 deaths have been declared as unlikely to be related to the vaccine. How is this determined? What pathological findings are looked for? What sort of problems could synthetic mRNA, spike protein or lipid nanoparticles cause?
A substantial number of the reported deaths (58) are in limbo due to “insufficient information”. Does that mean someone is actually looking for the additional information or will they just sit there with no conclusion? What if all of those 58 deaths ARE due to the vaccine? That is more vaccine-related deaths than Covid deaths in NZ!
Who is assessing the risk-benefit ratio? At what point would the harm from the vaccine be considered too much?
How many sudden unexpected deaths in NZ teenagers have there been this year, and how do this year’s figures compare to previous years?
The Citizen’s Database has recorded a lot more potential vaccine related deaths – over 300. This is a collection of deaths that someone (a close family member, a more distant family member, a friend or a member of the public) has suspicions about. Usually these are sudden and/or unexpected deaths that occur shortly after a vaccination, or follow an illness that started following the vaccination. In many cases, they have not been reported to CARM as they have been dismissed by relatives and/or by doctors.
This database of New Zealanders who have died suspiciously close to vaccination has been provided on four occasions to Government officials with a request to investigate further. On only one occasion has receipt of this database been acknowledged, and it appears no action has been taken.
True, robust safety monitoring would investigate all these deaths, and every other death in a vaccinated person. This would be the case for other new medications.
Serious Adverse Events
With regards to the serious adverse reactions – strokes, heart attacks, pancreatitis, neurological disorders, Bell’s palsy, myocarditis – how many Kiwis should be allowed to be damaged before someone says ENOUGH! So far there are over 2000 reports, and ‘Continue to Monitor’ seems to be the official position.
What is happening in our hospitals? A New Zealand Herald article on the 2nd December 2021 (20) reported Hawkes Bay Hospital had postponed 21 elective surgeries over the previous two days, as it responded to a surge in hospital admissions. On the 10th December 2021 the headline was “ED is going to break” (21). It can’t be winter illnesses since it is summer, and it’s not Covid. Could it be due to vaccine adverse events? Could there be an increased number of strokes, heart attacks, blood clots, neurological disorders and other medical events filling our hospitals, as a result of the vaccine program?
It sounded similar in Dunedin. On December 8th, the NZ Herald (22) reported that Dunedin Hospital recently almost called a Code Black, meaning the hospital was full to capacity and there was no more room. According to the report there was no Covid in town, there was no seasonal flu, there was no bad weather, there was no long weekend and there were no car crashes. What was filling up the hospital? Could it have been adverse reactions to the vaccine?
The mainstream media have proved to be ineffectual and impotent when it comes to asking the real questions. Perhaps a true investigative journalist could find out why our hospitals are filled to overflowing.
How many miscarriages, stillbirths (particularly mid trimester ones), neonatal deaths and birth defects were there in New Zealand in 2021, compared to previous years. Apparently, there have been no links between the vaccine and miscarriage, stillbirth or neonatal deaths reported BY Medsafe.
However, there won’t be reports coming OUT of Medsafe about adverse events in pregnancy if the adverse events aren’t being reported TO Medsafe or CARM in the first place. EVERY pregnancy loss, neonatal death or birth defect in a vaccinated woman should be reported to Medsafe. Has this happened?
The Medsafe datasheet for Comirnaty (23) states: “There is limited experience with use of COMIRNATY in pregnant women. … Administration of COMIRNATY in pregnancy should only be considered when the potential benefits outweigh any potential risks for the mother and foetus.”
That surely means a personalised risk-benefit assessment should be done for each pregnant woman. Why have pregnant women all been told that this vaccine is perfectly safe at any stage of pregnancy?
Can a true investigative journalist please find out the actual numbers of pregnancy losses in New Zealand this year and their vaccination status? Have all adverse outcomes of pregnancy in vaccinated women been reported to CARM/Medsafe?
Structure of the Rollout
The structure of the vaccine rollout is interesting. It has mostly involved mass-vaccination clinics and has been separated from General Practice (GP) where there are already good immunisation systems set up and where the doctors and nurses generally know the medical histories of their patients and know how to contact them. There has been dissatisfaction in GP circles regarding this separation.
At a mass-vaccination clinic, the nurse or other person administering the vaccine, does not know the patient or anything about their medical history. They will likely never see the patient again. They won’t ever know what happened following the vaccination. They won’t see the adverse reactions from the injections they are administering. How many of the nurses giving the vaccines have followed up what happened to the recipients? How much illness, and how many strokes, heart attacks and deaths have followed the injections they have administered?
On the other hand when a patient turns up to the GP with an adverse reaction, it won’t be top of the mind for the GP or the practice nurse to consider the vaccine, as they have not been involved in its administration. The vaccine record does arrive quickly in a doctor’s inbox but a conscious effort is needed to go and look there to see when it was administered. If the GP or nurse had been involved in the process, it would likely be more obvious that one event followed the other.
Why was it structured like this?
Censorship
It seems there is no public discussion allowed about what many people in New Zealand know is happening. By now nearly everyone in this country knows at least one person who has had some medical event happen to them following this vaccine. Some people have several friends and/or family members who have had severe or ongoing long-lasting problems following the vaccine.
NZ is hearing from a handful of ‘experts’, many epidemiologists or academics (with potential conflicts of interest as they are working for a University or the Government or receive funding from pharmaceutical companies) rather than unconflicted doctors with clinical experience who are seeing real patients on the ground.
Most of the ordinary doctors who have spoken publicly voicing concerns about adverse effects, or voicing an opinion that is not in line with the Ministry of Health’s official narrative, have either had their Practicing Certificate suspended (24) or are being threatened by the MCNZ (Medical Council of New Zealand) with suspension of their Practicing Certificate.
Why are New Zealanders not allowed to hear from doctors and scientists who have different opinions, perspectives or solutions?
Conclusion
In conclusion we are being told a vaccine is the only option. We are being told it is safe and effective. It has been given to millions of people. However, it is new technology, the clinical trials are not yet completed, the vaccine only has provisional consent, Pfizer is providing ongoing safety data to Medsafe, many New Zealanders are experiencing medical events in the days or weeks following vaccination, many of these potential adverse events are not being reported, our reporting system is under pressure, it is not clear who is assessing the adverse event data, our hospitals are mysteriously full in summer, and it is not clear when anyone will say “ENOUGH, the risks outweigh the benefits”.
It is time to call a halt to the vaccination program and have these concerns addressed in a thorough and transparent way by the Ministry of Health, the Director General of Health and the Prime Minister.
References
- https://www.nejm.org/doi/full/10.1056/nejmoa2034577 Initial Pfizer study in NEJM
- https://clinicaltrials.gov/ct2/show/NCT04368728 Clinical Trials ongoing until May 2023
- https://gazette.govt.nz/notice/id/2021-go338 Original 58 conditions of Provisional Consent
- https://www.medsafe.govt.nz/COVID-19/Comirnaty-Gazette-Oct-2021.pdf Eight conditions of renewed Provisional Consent
- https://www.medsafe.govt.nz/profs/PUarticles/DES2006.htm Diethylstilboestrol
- https://medsafe.govt.nz/Profs/datasheet/c/comirnatyinj.pdf Comirnaty Medsafe Data Sheet – Safety in Adolescents, 4th paragraph page 6
- https://clinicaltrials.gov/ct2/show/NCT04816643?term=Study+C4591007&recrs=ab&draw=2&rank=1 Clinical Trials showing C4591007 not completed until 2026
- https://www.medsafe.govt.nz/Profs/Datasheet/c/Comirnaty0.2mlOrangeCapinj.pdf Medsafe Data sheet for children 3rd paragraph page 6
- https://www.fda.gov/media/153409/download VRBPAC meeting Briefing Document Oct 2021 – not enough data re myocarditis 3rd paragraph page 12
- https://www.medsafe.govt.nz/profs/PUArticles/ADRreport.htm only 5% adverse events reported
- https://covid19.govt.nz/covid-19-vaccines/how-to-get-a-covid-19-vaccination/what-to-expect-when-you-get-your-vaccinations/side-effects-of-covid-19-vaccines/ Expected adverse events MoH
- https://medsafe.govt.nz/safety/Alerts/covid-19-vaccination-in-pregnancy.asp no pregnancy concerns
- https://medsafe.govt.nz/safety/Alerts/COVID-19-vaccine-blood-clots.asp no concerns re blood clots
- https://medsafe.govt.nz/safety/Alerts/comirnaty-menstrual-disorders.asp no menstrual concerns
- https://medsafe.govt.nz/safety/Alerts/comirnaty-myocarditis.asp Myocarditis as potential adverse reaction
- https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2020-10/COVID-Anderson-508.pdf Slide 16 adverse effects to watch for
- https://www.medsafe.govt.nz/COVID-19/safety-report-39.asp Safety Report 39
- http://web.archive.org/web/20211108125607/https://www.medsafe.govt.nz/COVID-19/monitoring-process.asp Methods not Finalised
- https://www.medsafe.govt.nz/COVID-19/monitoring-process.asp current safety monitoring methods
- https://www.nzherald.co.nz/hawkes-bay-today/news/hawkes-bay-hospital-postpones-21-elective-surgeries-in-two-days-as-admissions-soar/L7H3CR2M73PZRS64IUGHFXQNOE/ HB Hospital Full
- https://www.nzherald.co.nz/hawkes-bay-today/news/ed-is-going-to-break-hawkes-bay-hospitals-senior-most-ed-nurses-say-its-not-prepared-for-summer-covid-outbreak/T5ABADZHMSG6T7KVBKGXNLYRH4/ HB ED Going to Break
- https://www.nzherald.co.nz/nz/dunedin-hospital-close-to-code-black-full-capacity/L5LX3EXNSVDBFYCESSKB5GGDQM/ Dunedin Hospital Full
- https://medsafe.govt.nz/Profs/datasheet/c/comirnatyinj.pdf Section 4.6 re pregnancy
- https://www.rnz.co.nz/news/national/457915/covid-19-misinformation-probe-three-doctors-suspended-from-practising Doctors Suspended Amid Misinformation Probe