Evidence of Dishonest Claims About C-19 Vaccines and Reproductive Health as Alarming Safety Signals Emerge: Further Damning Data

Further Damning Data on Reproductive Health 22 February 2023
We repost and update this important article, initially published on 27 October 2022, to include a new interview (OBGYN reveals damning data on miscarriage and fertility rates in bombshell interview) with another specialist describing the increased miscarriages and decreased fertility following the genetic injections. She deals further with the nonsense spouted to persuade pregnant women to get jabbed. Remember, through mandates, some of these people were literally forced, on pain of unemployment.
[Updated 31st October 2022 to reflect new data released under NZ’s Official Information Act]
Reproductive Health
Since the genetic injections were rushed out and side effect reports began flooding in to the American VAERS database, the effects on pregnancy, reproduction and menstruation have stood out and yet been universally ignored and dismissed by authorities, along with the many other adverse events, often catastrophic.
Substack blogger and research philanthropist Steve Kirsch has interviewed obstetrician James Thorp on his findings, as profiled on this very good research summary by Etana Hecht. She also highlights the heroic work of women’s health champion Dr Naomi Wolf, whose team of thousands is sifting through the court-ordered Pfizer documents to uncover egregious harm. Steve has posted his own update article which includes the following dramatic comparison with reports of lost babies after all prior vaccines, from the new page on reproductive health events on OpenVAERS.

Steve points out that prior vaccines have been pulled immediately after much fewer side effects; that mainstream media and authorities are completely silent on this catastrophe; and the numbers reported are very likely a dramatic under-estimate of the true picture.
We have raised these concerns also, and documented them repeatedly at NZDSOS.com. Recently a supporter investigated and documented the timeline of what was claimed and when, by the New Zealand government, against documentation showing what was actually known. No prizes for suspecting a disconnect.
In recent months, alarming safety signals have emerged out of Germany, Hungary, Sweden, Switzerland, Iceland, the UK and Taiwan with regard to 2022 Q1 birth data. There is not usually much variation from year to year but the drops in 2022 Q1 are statistically unprecedented. Q1 2022 birth data relates to conceptions between March and June 2021 which, for the most part, preceded the mass vaccine rollout in the reproductive population. Q2 data is anxiously awaited worldwide to see if the downward trajectory continues.
Female Reproductive Health
Examination of the Risk Management Plan (RMP) submitted by Pfizer as part of the provisional approval process shows in Table 1 that use in pregnancy and while breastfeeding is “missing information”. Table 5 of the RMP outlines ongoing pharmacovigilance activities with regard to use in pregnancy.
There is only one trial related to maternal vaccination registered so far in the U.S. National Library of Medicine clinical trial database. This is Trial C4591015 which involves 349 participants, now in the collation, analysis, reporting and publication phase. The most long-term primary endpoint for this study is monitoring adverse effects until 6 months after delivery.
As per table 11 of the RMP the remainder of these studies are still underway and are not registered in the U.S. National Library of Medicine. Doesn’t this mean that all pregnant women receiving vaccinations as health interventions are actually trial participants?
| C4591009 | in the general US population within selected data sources participating in the US Sentinel System (FDA’s national electronic system) |
| C4591010 | in the real world. |
| C4591015 | Completed July 2022. Now in the collation, analysis, reporting and publication phase. The most long term primary endpoint is monitoring adverse effects until 6 months after delivery. |
| C4591021 | in the real world |
It appears that the studies meant to reassure us that the vaccines are safe and effective for pregnant women in the general population remain incomplete, in 3 out of 4 cases, while we are being told by our authorities that Covid-19 vaccines are safe and effective! The only study which is complete involved 349 trial participants, which is statistically insignificant – miniscule frankly – for a vaccine being administered to millions of pregnant women and billions of women of reproductive age.
From NZ Govt’s Unite Against Covid-19:
From Ministry of Health:
Study C4591015 will not capture adverse events beyond 6 months after delivery. In New Zealand, primary care and hospitalisation data is provided to Helen Petousis-Harris’s GAVI-funded Global Vaccine Data Network. Whilst this will provide for longer term capture of adverse events there is no indication that it will be public-facing or available for independent analysis. Petousis-Harris also advises Pfizer according to Dr Guy Hatchard, which is a clear conflict of interest. Read more on this at ‘The Curious Case of the Gates Foundation, the US CDC and Our NZ Health Data‘.
As recently evidenced by Dr. William C. Gruber, Senior Vice President of Pfizer Vaccine Clinical Research and Development, it is unknown how much spike protein is produced after mRNA vaccination and for how long. Operation Warp Speed saw to that. At 3 hours:10 minutes in to the FDA’s June 2022 Vaccine and Related Biological Products Advisory Committee (VRBPAC) meeting on 15 June 2022 Dr Gruber cannot or will not say how much spike protein will be made by the body after Covid vaccination, or how persistently.
An Israeli study on Covid-19 Vaccines and Ovarian Reserve is currently in the data collation to publication phase. It is not due for release until February 2024. Vaccinated women considering whether and when to start a family shouldn’t have to await this data.
From a useful Natural News article, this reminder:
“Buried in the Pfizer documents is an important observation on pregnancy loss. Of the 34 known pregnancies exposed to Pfizer covid-19 vaccination prior to February 2021, a total of 23 ended in spontaneous abortion! Another two pregnancies ended in premature baby death; two were ruled intrauterine death; one was a neonatal death; and five had a pending outcome. Out of the 34 cases, only one of the pregnancies had a normal outcome.”
Do not forget that the outcomes of 238 more women who conceived during the trial were “unknown” to Pfizer. This is pivotal data, surely! How hard did they try to follow them up?
Dr James Thorp, a maternal-fetal medicine expert, has reported VAERS data related to Covid-19 vaccines and compared them to VAERS data for influenza vaccines. His preprint analysis is to be published in a medical journal but Epoch Times wanted to disperse his findings with haste:-
- Abnormal uterine bleeding (menstrual irregularity) is 1000-fold greater
- Miscarriages are 50-fold greater
- Fetal chromosomal abnormalities are 100-fold greater
- Fetal malformation is 50-fold greater
- Fetal cystic hygroma (a major malformation) is 90-fold greater
- Fetal cardiac disorders are 40-fold greater
- Fetal arrhythmia is 50-fold greater
- Fetal cardiac arrest is 200-fold greater
- Fetal vascular mal-perfusion is a 100-fold greater
- Fetal growth abnormalities are 40-fold greater
- Fetal abnormal surveillance tests are 20-fold greater
- Fetal placental thrombosis is 70-fold greater
Adding his own experience to his research, this eminent, sober medical professional states: “I have witnessed many, many, many complications in pregnant women, in moms and fetuses, in children, offspring […] what I’ve seen in the last two years is unprecedented“.
He says the numbers reported amount to “severe safety signals“. “It’s way off the charts“, he said.
Dr Thorp has recently roasted New Zealand GP Dr Nikki Turner of the Immunisation Awareness Centre. In very strong language he severely criticises her endorsement of the Pfizer product to women of child-bearing age, in a two-part interview with Counterspin Media (episode 75; episode 76). He accuses her of capital crimes. We await her response with interest.
Counterspin have recorded an interview too with a New Zealand GP who calmly talks us through official documents giving contradictory advice to doctors, as well as talking to a midwife who cannot stay silent on the harm that she is witnessing.
Male Reproductive Health
Whilst Ministry of Health and Unite Against Covid-19 publish reassuring material on the safety of Covid-19 vaccines in pregnancy there is a distinct absence of safety material specific to male fertility from those sources. The decline in birth rates being seen in countries with high vaccination rates, comparable to New Zealand, are not yet capturing any potential effects of Covid-19 injectable products on male fertility. If those effects exist, the consequences should be evident very soon in data from fertility clinics.
Prior to going to market Pfizer did not test ‘male reproductive toxicity’, defined as adverse effects of the injections on adult male sexual function and fertility. Adverse effects from vaccinated men’s semen on the development of their offspring was not tested either. Further, the men in the initial ‘formal’ trial (as opposed to the billions injected subsequently in the ‘real world’ trial) had to agree to avoid intercourse for 28 days after each jab.
That these points were not made clear to New Zealand men as part of an informed consent process has denied men the ability to properly choose, and made them unwitting participants in an ongoing clinical trial of a novel gene therapy. Here again, as we always state, vaccinators broke codes of ethics in administering the jabs.
Post marketing documents from Pfizer made available by court order do raise concerning questions regarding male fertility. Condition 53 of Medsafe’s Provisional Consent to the Distribution of (BNT162b2) a New Medicine required provision of the six month analysis data from C4591001. In April 2021 Medsafe expected and received the report ‘5.3.6 Cumulative Analysis of Post-authorisation Adverse Event Reports of PF-07302048 (BNT162b2) Received Through 28 Feb-2021’. This OIA clarifies that Medsafe received this data in a New Zealand specific format. Although it doesn’t specify when, condition 57 of the original provisional consent expects Pfizer ‘to provide monthly safety reports, as well as all safety reviews they conduct or become aware of’.
So, this information was received by Medsafe prior to renewing the Provisional Consent for Comirnaty on 28 October 2021 and before the introduction of vaccine passes and non-border employment mandates in New Zealand. It includes ‘anti-sperm antibody positive’ as one of many Adverse Events of Special Interest in Appendix 1. Oh, and let’s not gloss over the 1223 deaths, and 40,000 side effects.
On June 22, 2022, the men’s health journal Andrology published ‘Covid-19 vaccination BNT162b2 temporarily impairs semen concentration and total motile count among semen donors.’ The study, which did not include the effects of booster injections, showed a worrying drop in male fertility, with an average decrease of 15.4% sperm concentration and 22.1% total motile count across the study group, from the 2 primary course doses alone.
Despite the word ‘temporary’ in the title, at close to six months post-vaccination, sperm concentration, motility, and total motile count were all still in significant states of decline versus pre-vaccination levels. Sperm concentration had not recovered at all and was, in fact, at its lowest point yet.
As the study was only done in those with 2 primary doses we do not know if boosters will have an even stronger negative impact on male fertility.
Perinatal Losses at Home and Away
A recent Substack article by data analyst Igor Chudov, CDC Data: Moderna Causes 42% MORE Miscarriages Compared to Pfizer, highlights multiple issues relating to data collection and analysis, and safety concerns, of Covid-19 vaccination in pregnancy. He links to information provided in a September 2021 Substack by medical blogger Arkmedic, The curious case of the miscalculated miscarriages which also highlights inconsistencies in data analysis.
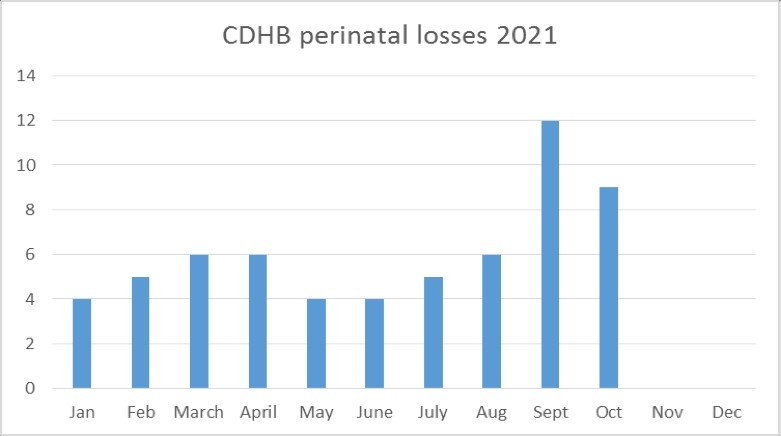
In New Zealand the response to OIA request CDHB 10746 covers a period too early for the dramatic September 2021 rise in perinatal death to be discussed in relation to the effects of Covid injectable products on male fertility. It will be very interesting to examine further data on perinatal deaths from the time vaccination in men of reproductive age could potentially have had an effect – particularly in the South Island whose population was Covid-naïve until January 2022 but where injection with Covid products started in July/August 2021 in men of reproductive age en masse.
Injection of the Covid-naïve pregnant women commenced in June. Note the sudden spike in dead babies 3 months later. No further figures are yet available.
To date 2021 figures (January – October 2021) Fig 5
Responses to other OIA requests do not reassure either. Stillbirths in Waikato, Lakes/Rotorua and Nelson/Marlborough DHBs had already easily exceeded the 2021 totals by June this year. The Perinatal Mortality and Morbidity Review Committee (PMMRC) was questioned by a concerned midwife (not the same one interviewed by Counterspin, above). She says:
“I have been assured they are ‘looking at it’. But given they haven’t even released their report for the 2019 data I won’t hold my breath [..] Early on in the rollout I asked the PMMRC if they would be including covid vaccination as a datapoint in their data collection. They said they were ‘looking at it’ but I never got confirmation. [..] All the DHB’s said they were not involved with any postmarketing pharmacovigilence for the vaccine in pregnant women. When Dr Nicky Turner gave her IMAC webinars to medical staff at rollout’s start, including to midwives, she assured that our women would be followed in ongoing studies. There are none.”
Like Dr Thorp, we have to ask: did Dr Turner lie?
BBC News reports that Scotland is to investigate two spikes in newborn deaths that have occurred since the injections. These baby deaths are currently at the highest levels they’ve been at in 10 years. However, they don’t intend to assess vaccination status of the mother as a variable of interest. Dr Sarah Stock, a maternal-foetal medicine specialist at Edinburgh University and co-leader of the Covid-19 in Pregnancy Scotland (COPS) study, is quoted as saying that whilst it was known the virus can cause pregnancy complications, simultaneously the Covid vaccine is not a factor in these deaths. How does she know? Where’s her data?
Dr John Campbell discussed the increase in newborn deaths in Scotland in 2021 and 2022 in his 20 October 2022 video. In a population of 5.5 million, Scotland saw spikes in September 2021 and March 2022 of more than double the average expected neonatal deaths. He notes too that public health experts have ruled out covid-19 itself as the cause, but refused to investigate the maternal vaccination status related to these deaths, and they claim that there is “no plausible reason to do so, due to the potential for harm to vaccine confidence”. So there we have it: finally, an honest statement.
Campbell discusses also that distressed parents are reporting that their babies who die shortly (including up to five days) after birth are being deliberately misclassified as stillbirths (born dead). This removes them from the remit for coroner scrutiny. Why would authorities want to do that?
Vaccine Appears in Breastmilk
Quoting from Etana’s blog, “Last month, the Journal of the American Medical Association published a report confirming that mRNA is found in breast milk.
This is also the first high-profile report that admits what Pfizer knew back in 2020 – that there is biodistribution of the vaccine ingredients throughout the entire body, contrary to what the world was told.
Though they stopped short of recognizing the danger of vaccinating mothers altogether, and simply recommended that women refrain from breastfeeding for two days after vaccination, the high-profile confirmation of DailyClout’s findings is a bombshell that should be making headlines across the nation. Dr. Wolf pointed out that JAMA’s conclusion that breastfeeding mums should wait two days before nursing is dangerous to women and babies since one of the dead babies in the VAERS database died fourteen days after the mother’s vaccination.”
Our Pfizer cheerleader Dr Nikki Turner, who so incensed the vastly experienced Dr Thorp, tells us in her government ads that it is a good thing that mum’s antibodies pass to the baby, but we wonder if she feels the same way about the lipid nanoparticles in the milk, given that no nation has approved the jabs for newborn babies. But then, she may be unfazed, having previously marketed the vial contents as a little piece of genetic material wrapped in a fatty bubble, some salts and sugar products, as we bellyached about in our complaint to the Broadcasting Standards Authority. Our complaint was not upheld.
Biodistribution and Spike Protein Replication/Persistence
The narrative was always that materials injected in mRNA vaccines remained at the injection site and near local draining lymph nodes in order to activate the immune system. Dr Byram Bridle in Canada applied for an FOI through the Japanese regulatory agency and in late May 2021 obtained a biodistribution study done in animals.
This study is evidence the lipid nanoparticles (LNP), the carriers of the mRNA, do get into blood circulation and distribute widely. In the study was evidence of accumulation in the tissues of the spleen, bone marrow, liver, adrenal glands, and ESPECIALLY MARKED in the ovaries for up to 48 hours. After that the animals were terminated so there is no indication as to how long accumulation went on.
There is still no data on what effect the accumulated LNPs and the modified spike protein will have on the ovaries and other sites where LNPs have accumulated. But there are some alarming signals in the adverse event reports, damningly ignored in lockstep by all the big ‘stakeholders’.
A July 2021 OIA requested provision of pharmacokinetic documents the New Zealand Government received, and documentation and evidence to support the following claim made by the Ministry of Health:- ‘No parts of the vaccine or the spike protein produced reach the ovaries or the testes.’
The OIA request was partially successful, in that a response on 5 August 2021 (H202108426) withheld release of the pharmacokinetic documents citing protection of the commercial position of the supplier of the information. The source of advice for the statement regarding distribution of the vaccine or spike protein to reproductive organs was cited as www.covid.immune.org.nz, the website of Immunisation Advisory Centre (IMAC). The OIA response acknowledged that upon review subsequent to the OIA request, the statement regarding spike protein or vaccine ability to reach testes or ovaries would be removed from the Ministry of Health website. A rare and small victory for unsullied data, but no warning or caution replaced the misleading statement that was removed.
Reverse Transcription
All the so-called “experts” were universal in their scorn against our concern that mRNA might become integrated into the cellular DNA, despite clear pathways for that to happen. A study published 25 February 2022 shows the messenger RNA in the Pfizer BioNTech mRNA vaccine, when injected human liver cells, converts into DNA, potentially hard-coding instructions for the cell. Like Pfizer’s nonsense that the injection would stay in the arm muscle, it was also promoted that reverse transcription into DNA would not happen, but it can – and fast. Within 6 hours the DNA was into the liver cells’ nuclei. Rapid uptake of BNT162b2 increases expression of a protein called line-1 and causes changes to its distribution. A further study has found that either too much or too little line-1 expression can cause embryo development to come to a halt. Alarm should be mounting in high places.
Spike protein expression in the liver cells was also observed which would make cells a target of the immune system and could potentially cause autoimmune hepatitis. (Remember the curious outbreak of viral hepatitis amongst children too young to be vaccinated, but mostly breastfed by vaccinated mothers?) There is also concern that the RNA entering the cell’s nucleus could integrate with DNA and cause genomic toxicity leading to cancers. If RNA can enter the nucleus of in vitro liver cells, what else can it do?
What is not known with certainty is whether the DNA created integrates permanently into the genome.
Further explanation of this study can be found here.
Yet the Unite Against Covid-19 and Ministry of Health are still claiming that the mRNA from the vaccine will not enter the nucleus of cells. It is not yet known the extent to which RNA could enter the nucleus of cells in a human body. Which cells, how many, will it happen in everyone – all that is unknown. But it can not now be said that the vaccine will not enter the nucleus of cells because we know that it can.
All of this is extremely concerning, to say the least. It points at best to a gross dereliction of duty and/or corruption of our regulators, and at worst, to a disastrous crime of inestimable proportions. The injections must be stopped immediately.
Further NZDSOS Information About Reproductive Health Concerns:
- Pfizer Trials Show Catastrophic Impact on Human Fertility: Comprehensive Reports From Investigative Research-Journalist Collaboration
- Covid-19 and Fertility: Why Are Fewer Babies Being Born?
- COVID-19: The Unraveling of Experimental Medicine and The Golden Rule of Pregnancy